Insights for clinical leaders, physicians, nurses, and care teams focused on improving care delivery, reducing administrative burden, and enhancing the clinical experience.
How Intelligent Care Enablement Platforms Streamline Transitions of Care
Commure Team
|
October 3, 2025
Care doesn’t end when the IV comes out and the telemetry monitor is silenced. Once patients leave the hospital, most of their recovery plays out at home, where daily choices and limited support determine whether care plans hold or drift. The journey spans far more than a series of visits, and the handoff between settings shapes everything that follows.
For years, the default response was to add people and stretch shifts to cover every detail of discharge. Unfortunately, that approach almost always breaks down under staffing shortages, constrained resources, and slipping engagement.
What is needed now is a smarter layer of support that helps teams guide patients through the days and weeks after they leave. With the right technology, instructions carry forward, risks surface sooner, and transitions become easier for patients and clinicians to navigate.
What are transitions of care, and what are the risks?
Transitions of care are the handoffs between settings in a patient’s journey, like discharge from the hospital, a move to rehab, or the shift to at-home care. These moments are vulnerable. One study found that nearly 20% of patients experience adverse events within three weeks of discharge.
Another large contributor to failed transitions is handoffs between providers. One study showed the likelihood of 30-day hospital readmission increases by 16 percent with just a single handoff, and one in four hospitalizations during home health care could be avoided if handoffs were eliminated.
When handoffs falter, care teams feel the strain. Workloads rise, scarce resources get stretched, and frustration grows as avoidable issues return to the front door. The result is less time for top-of-license work, weaker communication, and a higher chance that small problems escalate into patient harm.
How can transitions of care be improved?
To fix transitions, start with why they break down. Discharge information is often incomplete or hard to follow, which leads to missed medications, drift from the care plan, and preventable readmissions.
The strongest lever to combat this breakdown in care is standardized, clear communication at discharge and across settings. Studies have found that communication interventions at the point of discharge are strongly associated with fewer readmissions, as well as better treatment adherence and patient satisfaction.
However, conversation alone is not enough because patients forget more than 50 percent of what is discussed. It is important to reinforce instructions with timely reminders and anticipatory guidance delivered where patients will actually see and use them.
How can digital healthcare help with transitions of care?
Closing the gap after discharge takes more than a conversation at the bedside. An intelligent care enablement platform gives patients and clinicians continuous support as care moves from hospital to home. Here is how they can help:
1. Streamlining care coordination
A unified view of the patient’s journey helps teams act quickly and consistently. With Commure Engage, clinicians can see patient messages alongside history and prior touchpoints, then loop in the right colleagues from an EHR-integrated workspace so nothing gets lost between settings.
2. Automating care follow-up
Refills, check-ins, and reminders are essential yet time-consuming when handled manually. Automation ensures every patient gets timely outreach and symptom checks, while clinicians spend more time at the top of their license and less time chasing tasks.
3. Educating patients
Discharge education fades fast. Conversational AI keeps teaching alive after the hospital stay by answering plain-language questions, reinforcing critical steps, and guiding patients to next actions with clinically reviewed content.
4. Simplifying symptom management
New or confusing symptoms often drive unnecessary calls and readmissions. A virtual assistant can respond in real time, ask clarifying questions, and escalate to the appropriate clinician when needed, giving patients clear direction and care teams actionable context.
5. Improving remote patient monitoring
Once patients are home, visibility drops. SMS-based outreach meets people where they are, captures status through brief check-ins, and flags issues early. That reduces back-and-forth in portals, clears up miscommunication, and keeps transitions moving in the right direction.
Ready for smoother transitions of care?
Every organization has its own hurdles, but the fix begins with clear communication and a platform that keeps guidance consistent from bedside to home. Commure Engage was built to do exactly that, so patients land on their feet and care teams stay aligned.
Healthcare automation has already saved the US health system hundreds of billions of dollars. Electronic transactions and automation helped the industry avoid an estimated $258 billion in administrative costs in 2024, with roughly $21 billion a year still available from work that stays manual or partly manual, according to the 2025 CAQH Index.
The strain behind those figures shows up on every clinical schedule. Physicians reported a 57.8-hour workweek in 2024, and 7.3 hours of it went to administrative tasks like prior authorization, insurance forms, and meetings, per the American Medical Association.
For health systems looking to cut administrative costs and give staff time back, the real question is what to automate, in what order, and how to do it without adding risk.
What is healthcare automation?
Healthcare automation is the use of technology to complete healthcare tasks with little or no manual effort, across operational, financial, and clinical work. It covers everything from insurance eligibility checks and claims processing to clinical documentation and patient reminders.
Most people first meet it in its narrow form, robotic process automation (RPA) in healthcare, where software handles repetitive, rule-based steps such as data entry or eligibility verification. The broader term is intelligent automation, which combines RPA with artificial intelligence so systems can read unstructured documents, interpret context, and make complex decisions.
Health care automation works best when it runs across a whole process rather than one isolated step, so a patient's information moves from intake through documentation, coding, billing, and follow-up without being re-keyed at each stage.
The main types of healthcare automation
Healthcare automation spans a few distinct technologies, and knowing the difference helps you match the right tool to the right job.
Robotic process automation (RPA). Software bots follow fixed rules to handle high-volume, repetitive tasks like eligibility checks, claim status lookups, and moving data between systems. It's fast and reliable for work that never changes.
AI and machine learning. These models find patterns in data, so they can predict likely claim denials, prioritize worklists, or surface a possible diagnosis for clinician review. They get better as they see more examples.
Intelligent automation. This pairs RPA with AI so a single workflow can read a faxed referral, pull the relevant clinical details, and route the case, handling the messy inputs that rule-based bots alone can't.
Ambient AI. Ambient AI listens during a visit and drafts the clinical note in real time, which is why teams often ask how ambient AI and AI scribes differ. It takes documentation off the clinician's plate entirely.
Agentic AI. The newest layer, agentic AI, can plan and carry out multi-step tasks on its own, check its work against policy, and pull in a human when a case needs judgment.
You don't have to pick just one. Most decisions here land with the people accountable for operations, revenue, and IT, so whether you're a COO weighing throughput, a revenue cycle or finance leader watching cost per claim, or a CMIO protecting clinician time, the goal is the same. A mature program uses all of these types, matched to the risk and complexity of each task.
Where healthcare automation works across health systems
Healthcare automation can be applied across the entire care and revenue journey, not only the billing office. Health systems get the most from it when their automation connects these areas, so information flows from one to the next instead of stopping at department lines.
Patient access and intake. Automated scheduling, reminders, and digital intake reduce no-shows and cut front-desk phone volume, while eligibility checks confirm coverage before the visit. This is the front end of patient engagement, where modern patient communication software handles two-way conversations: reminders, replies, scheduling, and follow-up in one place. Yale New Haven Health used automated pre-visit outreach to cut no-shows and same-day cancellations by 54% in its breast imaging program.
Clinical documentation. Ambient AI drafts notes during the encounter, and dictation feeds structured data back into downstream systems, so clinicians spend less of the visit typing.
Patient communication and coordination. Healthcare AI agents handle inbound calls, answer routine questions, and manage follow-up, freeing staff for work that needs a human.
Back office. Supply chain ordering, compliance reporting, and security monitoring all run more accurately when automated systems handle the routine checks.
The core benefit of healthcare automation is time returned to people, which then shows up as lower costs, fewer errors, and a better experience for patients and staff.
When automation absorbs data entry, paperwork, and documentation, clinical teams spend more of the day on care and administrative teams move to higher-value work. At North East Medical Services, clinicians started heading home 1 to 2 hours earlier each day after adopting ambient AI.
Costs also drop and revenue holds. Fewer manual touches mean fewer coding and billing errors, faster payment, and less rework, which is how one New York City health system raised revenue cycle performance by 20%.
Patients notice too. Faster scheduling, quicker responses, and fewer forms make the experience smoother, and automated follow-up keeps people engaged between visits.
Automation also scales in a way that hiring can't. A system absorbs higher patient volumes without adding headcount for every task, and automated access controls and audit trails support compliance along the way.
What to automate first
Start where the burden is heaviest, and the payoff is fastest to see, then expand into adjacent work. Early, visible wins build trust that carries into the next project.
Clinical documentation is the clearest first move. It's the single largest source of clinician time and burnout, and ambient AI addresses it directly by drafting the note during the visit for the clinician to review and sign, so results show up right away in reclaimed hours and less after-hours charting. Because a clinician still approves every note, the clinical risk stays low while the relief is immediate.
Prior authorization is the next obvious candidate. Physicians and their staff spend about 13 hours a week on it, completing roughly 40 requests per physician, and 40% of practices now employ people who work on nothing else, according to the AMA's 2025 survey. It's high volume, highly repetitive, and directly measurable, which is exactly the profile automation handles well.
Eligibility verification, patient intake, claim scrubbing, and appointment reminders fit the same criteria and are common early wins.
Sequence matters as much as selection. Prove the value on one workflow, measure the time and money it returns, then expand into adjacent steps. A phased rollout produces the hard numbers you need to justify each next investment.
Why healthcare automation succeeds or stalls
Automation succeeds when it fits how clinicians already work, and it stalls when it's bolted on without their input. The technology is rarely the hard part; adoption is. A few practices separate the programs that stick from the ones that stall:
Bring staff in early. Involve the clinical and administrative teams who'll use the tools before you buy, so the workflow fits their day instead of fighting it.
Aim for top-of-license work. Target the tasks that pull people away from what they trained for, and measure success by the time given back, not screens added.
Keep a human in the loop. Let automation handle the routine work and route exceptions and anything with clinical or financial weight to a person for review.
Start small and prove it. Roll out one workflow, show the time and dollars it returns, then use those numbers to justify the next phase.
Get governance right from day one. Automated systems touch protected health information, so insist on HIPAA-compliant handling, clear audit trails, and attention to model bias.
Integrate with the EHR. Tight integration keeps data accurate and stops staff from re-keying information between systems.
Healthcare automation is now core infrastructure
Healthcare automation is no longer optional: health systems and mid-sized practice groups nationwide are treating it as a core part of how they operate and compete. The organizations seeing the greatest results treat it as one connected system, starting where the work is most repetitive and the ROI is hardest to ignore. The real opportunity lies in building automation that compounds, with each layer making the next one more powerful.
See how the Commure platform brings ambient AI, revenue cycle, and patient engagement together in one place.
Frequently asked questions
What are examples of healthcare automation?
Common examples include automated appointment scheduling and reminders, insurance eligibility checks, medical coding, claims processing and denial prevention, ambient AI that drafts clinical notes, and AI agents that handle patient phone calls. More than 50% of health plans and 25% of provider organizations now use AI in administrative workflows, per the 2025 CAQH Index.
What's the difference between RPA and AI in healthcare?
RPA follows fixed rules to automate repetitive tasks like data entry and eligibility checks, and it can't adapt on its own. AI uses machine learning to interpret data, predict outcomes, and handle unstructured inputs like faxed referrals. Intelligent automation combines the two, which is what most healthcare workflows actually need.
Will healthcare automation replace healthcare jobs?
No. Healthcare automation mainly targets administrative and repetitive work rather than clinical judgment, so it shifts staff toward higher-value tasks instead of eliminating roles. Physicians spend 7.3 hours a week on administrative tasks alone, per the AMA, and automating that work lets clinical teams operate at the top of their license.
Is healthcare automation HIPAA compliant?
It can be, when built correctly. Automation tools handle protected health information, so they need HIPAA-compliant data handling, encryption, access controls, and audit trails. Compliance depends on the vendor and configuration, not the technology itself. Commure is HIPAA-compliant and built for enterprise health systems, so hold any platform you evaluate to that same standard.
How do you get started with healthcare automation?
Start with one high-volume, rule-based, low-risk workflow such as prior authorization or eligibility verification. Measure the time and money it returns, then expand into adjacent steps. A phased rollout builds staff trust and produces the hard numbers you need to justify each next investment.
Tell us a little bit about yourself—what do you like to do outside of work?
Relocating from Long Island, NY, 5 years ago with my wife and 2 daughters, ages 8 and 6, to the Raleigh-Durham, NC area - there is no shortage of fun to keep us busy down here. From hiking trails at the lake to pickleball to dance class to the swim team, we are always keeping active. My daughters are slowly becoming “foodies” too. They don’t run with the chicken nugget and tater tot crowd. They love sushi and ramen. They love “millionaire” bacon (just add a little brown sugar) and “fruity-face” pancakes. We grill year-round - my kids are carnivores! - so my rib-eye steak and cheeseburger game is on point. North Carolina is known for its BBQ - we’ve tried many of the local places and think we found our go-to spot. We have also started baking together more - the kitchen gets wrecked, but we have a blast, and the end product is always worth it. Look up the recipe for Hummingbird Cake and thank me later.
As a kid, what did you want to be when you grew up?
I thought I wanted to be a doctor - then I took Organic Chemistry in college as a Pre-Med major…that's when I learned I didn’t really want to be a doctor. Whenever my kids need a band-aid, I’m quick to tell them: “Don’t worry, Dad was pre-med for a semester. You’re in good hands.”
I wound up studying Psychology and Sociology at the University of Notre Dame (Go Irish!), with intentions to pursue a career as a Sports Psychologist - but upon graduating instead received a wonderful opportunity in the Real Estate and Construction sector back home in New York City. This role afforded me an opportunity to work on many high-profile projects - many of which were engagements with large health systems such as NYU Langone Medical Center, Memorial Sloan Kettering, and Mount Sinai. My company at the time leveraged proprietary VR/AR software to design, manufacture, and build sustainable medical care spaces - everything from hospital headwalls and footwalls with embedded medical gases to millwork for nursing stations.
Describe a day in the life of your role.
As an Account Manager, serving as the single point of contact for our partners - the role touches every phase of every product in our bundle. A typical day looks like this: execute on whatever it is your partners require. We are full-time client advocates, relationship managers, issue-resolvers, account retainers, project coordinators, revenue and data analysts, product experts, process/workflow builders, strategic consultants, and often…behavioral psychologists!
What made you decide to join Commure?
From my time in construction, I learned this: demolition is easy; building is hard. Anybody can tear down or point out faults. The real skill and true craftsmanship is reserved for the creators and builders - people who take empty space and transform it into something beautiful and useful. Good design is both form and function, in harmony - the Commure product suite nails this.
Seeing firsthand the significant impact Real Estate and Facilities projects have on patient care - and a medical practice’s ability to generate revenue - laid the groundwork for pursuing a role at Commure to tackle the healthcare problem. The United States is #1 in the world in wealth, but outside the top 30 in healthcare delivery - this needs to change.
How would you describe the Commure company culture?
This is a team sport. While we each have distinct responsibilities, we operate as one team. Our culture is defined by collaboration, accountability, and a relentless focus on client outcomes. Across the organization, we are united by a common mission: building best-in-class, AI-native products to improve provider productivity, reduce administrative burden, and allow healthcare teams to focus on what matters most - patient care.
What advice would you give someone on their first day at Commure?
Be a heat-seeking missile for pain - actively seek the gnarliest challenges and pain points that impact our customers. Prioritize building product knowledge and expertise across our bundle. Operate without fear. Dive headfirst into ambiguous challenges, and when you identify a gap - the standing order to my team - go bridge the gap. You do not need to ask permission. Brick-by-brick, drive the company forward.
What has been your greatest accomplishment so far at Commure?
We have accomplished so much in my 2+ years - improving user experience while surfacing inconsistencies in claims before they were submitted - and fixing claims we knew an insurance company would deny payment before they were submitted. The impact of this release was astonishing - automating previously time-consuming workflows while improving First Pass Rate and cash flow for partners across our portfolio.
What does "a win" look like in your role?
Earning a renewal and extending into a multi-year partnership. It shows we have built trust, delivered meaningful results, and created an experience that our partners want to continue investing in. Those outcomes only happen when all disciplines - including Sales, Launch, Account Management, Operations, Engineering, Product, and Support - are working in harmony - one team. Every renewal strengthens our business and expands our opportunity to improve healthcare for more patients and providers.
Interested in a career building the next generation of healthcare technology powered by AI? We are always looking for talented people across our departments.
A new patient in one of the 15 largest metro areas in the U.S. now waits an average of 31 days to see a physician, according to AMN Healthcare's 2025 survey, and rural patients often wait longer still (roughly 20% of Americans live in rural areas while only about 9% of physicians practice there, according to the National Rural Health Association). That wait is a symptom of a system that loses patients before the patient journey ever begins, and every day of delay is a chance for someone to switch providers, defer care, or disappear from the schedule entirely.
The patient journey is the full arc of a person's experience with a health system, from the first symptom or online search, through treatment and long-term follow-up. Health systems have mapped that journey for years, yet far fewer have fixed the gaps along the way.
This guide covers what the patient journey is, the stages every patient moves through, how to map it, and how to close the gaps that quietly cost health systems patients and revenue.
What is the patient journey?
The patient journey is the sequence of interactions a person has with a healthcare organization over time, starting well before a first appointment and continuing long after a visit ends. It covers how someone finds a provider, books and prepares for care, moves through the visit itself, and stays connected for follow-up and ongoing needs.
Much of the healthcare patient journey plays out beyond the exam room: the phone tree at scheduling, the intake form, the reminder that does or doesn't arrive, the call after a procedure when a question comes up at 9 p.m.
It helps to separate two terms that often get used interchangeably. The patient journey is what actually happens to the patient. A patient journey map is the tool you build to see that experience clearly and decide what to change.
Why the patient journey matters
Healthcare has shifted from a system patients accepted to one they shop, and people now compare providers the way they compare any other service. That shift shows up plainly in switching behavior. About 1 in 5 patients switched providers in the past year, and nearly 90% of them did so because the organization was hard to do business with, according to an Accenture survey reported by the American Hospital Association. 7 in 10 pointed to access as a deciding factor when they chose someone new.
That pattern points squarely at the friction around care: the busy phone line, the confusing bill, the message that never gets a reply. Every one of those friction points sits somewhere on the patient journey, which is why mapping it and fixing what you find has become a retention strategy in its own right.
The stages of the patient journey
Most patient journeys move through 6 stages: awareness, consideration, access, the visit, follow-up, and ongoing care. Few patients travel them in a tidy line, since people loop back, pause, or drop out along the way, but the stages give you a shared structure for pinpointing where the experience breaks down.
Awareness
Awareness starts the moment someone notices a symptom or decides they need care. Most people begin with a search engine rather than a physician referral, so the clarity of what they find shapes their first impression of your organization long before they ever call. Content that answers real questions, a findable location listing, and current reviews all work well at this stage.
Consideration
In the consideration stage, patients weigh their options against practical criteria: location, accepted insurance, reviews, and whether they can actually reach you. This is where many patients silently choose a competitor, often for reasons that have nothing to do with clinical quality. A booking page that asks for too much, a call that goes to voicemail, or a week-long callback delay can end the relationship before it begins.
Access
Access is where the journey stalls more often than not. With new-patient waits averaging a month across major metros, the organizations that win patients are the ones that make scheduling fast and answer the phone reliably.
Access is also one of the more fixable stages. One community health center that began handling inbound calls with AI call center agents saved 800 labor hours for every 10,000 calls, roughly $240,000 a year, while resolving a large share of requests without staff involvement. Widening patient access at the front door keeps patients from giving up before they arrive.
Preparation belongs to this stage too. Long paper forms and prep instructions that are easy to miss create no-shows and day-of delays, which is why modern patient intake moves the clipboard onto the patient's phone through conversational outreach. Timely, multi-touch reminders that patients can actually respond to help reduce no-shows and protect both the schedule and the revenue attached to it.
The visit
The visit is where clinical care happens and where traditional patient-satisfaction measurement concentrates, spanning check-in, the encounter, and discharge. It's also where communication gaps take root, since patients often leave without asking the questions that mattered most to them and forget a large share of what they were told once they get home. What happens over the following days depends heavily on how well the visit sets them up.
Follow-up
Follow-up is the stage health systems most often let slide, even though it's where good clinical work can come undone. A 2026 study of more than 579,000 Medicare admissions found that many high-risk patients never receive post-discharge follow-up, and those who did were significantly less likely to be readmitted within 30 days. After a procedure, patients navigate medication questions, recovery uncertainty, and handoffs between care teams, and every handoff is a point where someone can slip through the cracks.
Two strategies make a measurable difference here. Tighter transitions of care keep information from getting dropped as a patient moves between settings, and proactive outreach closes the post-surgical care gap during the window when patients are home and most likely to need answers.
Ongoing care
Ongoing care turns a single visit into a lasting relationship that supports better health. For someone managing a chronic condition, this stage can stretch across years, and it's where loyalty is either earned or lost. Steady, personalized chronic care management keeps patients engaged between appointments, surfaces problems earlier, and reduces the avoidable complications that pull people back into acute care.
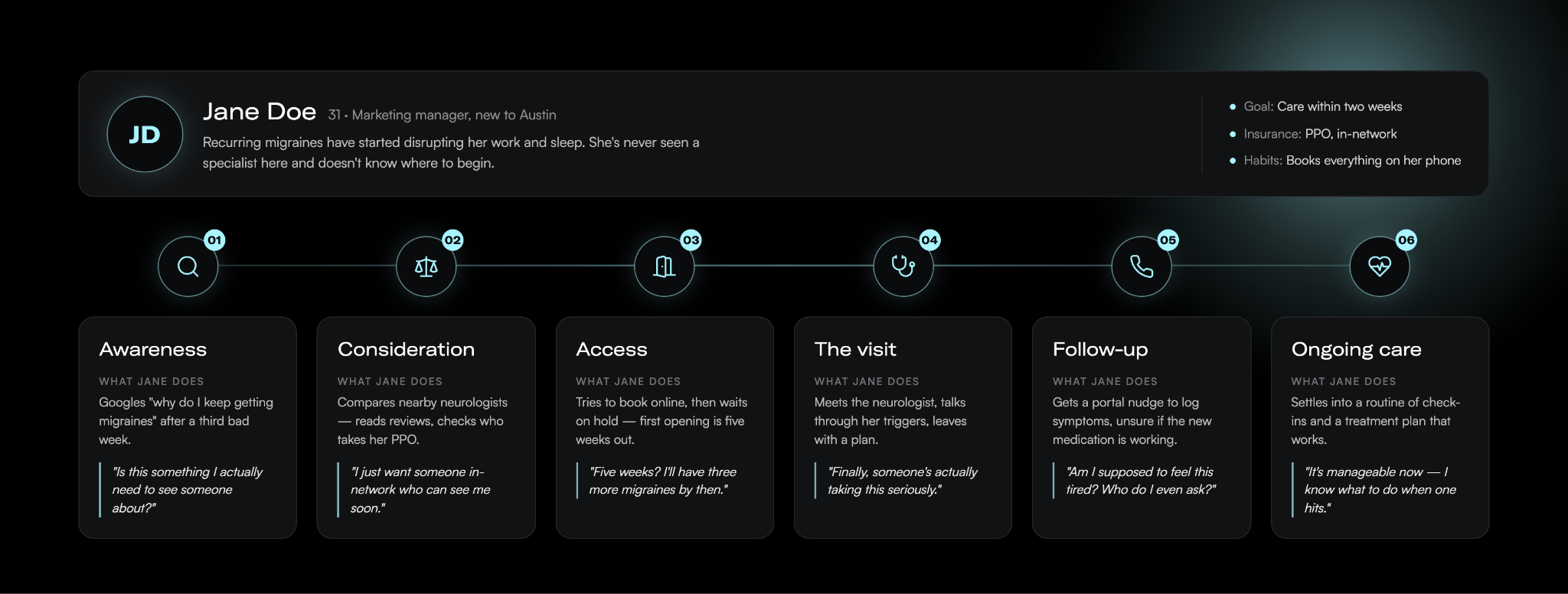
Patient journey mapping
Patient journey mapping is the practice of laying out each stage, touchpoint, and emotion a patient experiences, so you can see where the journey serves them and where it fails them. The patient journey map is the visual result, a shared picture of what patients do, think, and feel as they move through your system.
Here is a very basic example of a patient journey map. The more details you can fill in, the better.
Done well, a map earns its keep in a few ways. It creates a common view of the experience across departments that rarely talk to each other, exposes the specific moments where patients get stuck, and turns vague complaints about "patient experience" into a prioritized list of fixable problems.
Types of patient journey maps
Teams generally build one of four map types depending on the question they're answering.
A current-state map shows the journey as it runs today, drawn from real patient data, and it's the right starting point for incremental improvement.
A future-state map describes the journey you want to deliver and works well for aligning teams around a new service or process.
A day-in-the-life map widens the lens to what a patient experiences outside your system, which helps you spot unmet needs you'd otherwise miss.
A service blueprint goes the other direction and adds the people, systems, and policies behind each touchpoint, so you can trace a pain point back to the process that caused it.
Most organizations start with one type and add others as the work matures.
Patient journey analytics
The strongest maps sit on data. Patient journey analytics is the practice of layering your operational and experience data onto the map: scheduling and no-show records, call-center hold times, message response rates, portal usage, and post-visit feedback. Those numbers show you where patients actually drop off rather than where you assume they do, and they let you measure whether a change at one touchpoint moved the outcome you cared about.
How to map the patient journey
Here are the steps to take to build out your patient journey map:
Define your scope and goal. A map can zoom in on a single interaction, like booking an appointment, or span an entire condition, like managing diabetes over several years. Let the problem you're trying to solve set the boundaries.
Gather data from multiple sources. Combine direct patient input from interviews, surveys, and short diary studies with the operational and experience data you already hold, like scheduling records, message response rates, and existing patient satisfaction and engagement survey scores. Interviews add depth, surveys validate patterns at scale, and the data you already collect grounds the whole map in what really happens.
Build personas. A new mother's journey looks nothing like an oncology patient's, so segment by the populations you actually serve rather than mapping a generic average patient.
Chart touchpoints and emotions. For each stage, record what the patient does, who and what they interact with, and how they feel. The emotional low points usually mark your biggest opportunities, since that's where frustration leads to a decision to leave.
Validate and act. Put the draft in front of patients and frontline staff to catch what you missed, then commit to fixing the touchpoints it exposes. A map only pays off when it drives real changes to how you operate.
Common mapping mistakes
A few mistakes hurt the value of patient journey mapping. The most common is treating the finished map as the deliverable, when the map only matters once it changes how you work. Others include mapping the journey your organization wishes patients took instead of the one they actually take, building the whole thing from internal assumptions without talking to a single patient, and mapping so broadly that no team owns any specific fix. Assigning clear ownership for each stage, and revisiting the map as your services and patients change, keeps it from going stale.
Closing the gaps
Finding the gaps is the easy part; closing them, stage by stage, is where patient experience actually improves and where retention follows.
In practice, that means answering the phone during the access stage, replacing paper intake with conversational outreach before the visit, and staying in contact through follow-up and ongoing care instead of going quiet once the encounter ends. The connected set of tools that supports patients across all of these stages is what many health system leaders now call the digital front door, and it works best as a single platform that writes back to the EHR rather than a stack of disconnected point solutions. Keeping patients informed between visits is the job of patient communication software that reads each reply and routes anything a human needs to handle to the right person.
Commure Engage is built for exactly this work, supporting front-cycle patient experience across scheduling, intake, communication, and care navigation on one platform. Yale New Haven Health used Commure Engage for pre-appointment outreach in its breast imaging program and cut no-show and same-day cancellation rates by more than half.
Map the journey your patients actually take, then close the gaps one stage at a time. See how it all comes together.
What is the difference between the patient journey and the patient experience?
The patient journey is the full sequence of steps a patient moves through, from first symptom to ongoing care. The patient experience is how they perceive and feel about those steps. The journey is the path, and the experience is the quality of each interaction along it, which is why you map the journey to improve the experience.
What are the stages of the patient journey?
The patient journey typically moves through 6 stages: awareness, when someone notices a symptom; consideration, when they weigh providers; access, when they schedule and prepare; the visit, when care happens; follow-up, after a procedure or discharge; and ongoing care, which sustains the relationship over time. Few patients travel them in a straight line.
Who is responsible for the patient journey in a health system?
No single department owns the patient journey, which is part of what makes it hard to fix. It crosses scheduling, front-desk staff, clinicians, billing, marketing, and IT, so improving it takes shared ownership rather than one team's effort. Most organizations assign an owner for each stage plus a cross-functional group to keep the full journey aligned.
How can health systems improve the patient journey?
Health systems improve the patient journey by fixing the touchpoints a journey map exposes, stage by stage. The biggest gains usually come at access: answering the phone, offering online self-scheduling, and replacing paper intake with digital outreach. A July 2025 MGMA poll found 71% of practices have less than 25% of their patients using digital tools to self-schedule, so the opportunity is wide open.
When a clinic reaches a patient by phone before a visit, only 3% miss the appointment. When the reminder lands in voicemail, that climbs to 24%. When no one picks up at all, 39% don't show. Those numbers come from a study of 250 primary care patients managing depression, published in Psychiatric Services, and they point to something most communication tools get wrong. Reaching a patient and sending a message are two different things.
For 20 years, patient communication software has mostly meant reminders. An appointment gets booked, the system fires off a text or a robocall, and the office hopes it lands.
Modern patient communication software works differently. It's two-way, omnichannel, automated, HIPAA-compliant, and EHR-integrated. Instead of sending a text and hoping the patient receives it, AI reads each patient's reply, responds in natural language, and routes anything that needs a human to the right person.
Why one-way reminders hit a wall
Reminders work, up to a point. A randomized trial published in AJMC tested three approaches: a reminder 3 days out, 1 day out, or both. Patients who got both missed 4.4% of appointments, compared with 5.8% and 5.3% for a single reminder 3 days or 1 day before.
In that same research, the highest-risk group still missed roughly 20% of visits even after two reminders. The authors concluded automated messages have to be backed by staff outreach or patient navigation to engage with those patients.
So the old model forces a hard choice. Send more reminders that high-risk patients already skip, or put staff back on the phones.
A modern patient communication platform closes that gap. Automated digital care pathways are personalized to patients' unique care journeys, and AI call center agents can handle the follow-up calls that used to eat staff hours. One FQHC saw its agents save 800 labor hours for every 10,000 calls, about $240,000 a year.
What modern patient communication software actually does
Modern platforms respond, instead of just sending. When a patient texts a question, AI reads the reply and answers in plain language, drawing on a clinician-curated knowledge base, so responses stay inside vetted clinical boundaries. Anything urgent, or anything the system shouldn't answer on its own, routes to the right care team member.
None of this requires a portal login or an app. The platform reaches patients by SMS, RCS, voice, or email, and every exchange writes back to the EHR so the care team sees it where they already work.
Routine outreach runs on its own. Appointment prep, reminders, and post-visit check-ins go out automatically, without staff sending them one by one. The result is one continuous conversation with each patient instead of a scatter of one-way pings.
How to evaluate patient communication software
When you compare platforms, four things separate one that works from one that adds cost. Here’s what to ask when comparing vendors:
Ask whether it's genuinely two-way and omnichannel. A tool that only pushes messages out is a reminder system with a new name, and it leaves you managing the same problem you started with. Confirm patients can reply on the channel they choose and get a real answer back.
Ask how it handles HIPAA. A two-way thread carries symptoms, medications, and test results, so it needs the safeguards the HHS Office for Civil Rights expects: encryption, consent capture, access controls, and audit logging, with a business associate agreement in place. Get the specifics, not a compliance logo.
Ask how deep the EHR integration goes. Read-only isn't enough. Communication should write back to the record, or your care team ends up reconciling two systems by hand.
Ask where automation stops and people start. The platform should resolve routine volume on its own and escalate complex cases to staff, so you get the efficiency without dropping the patients who need a person.
These map to the broader questions health system leaders weigh when they build a digital front door, where communication sits alongside scheduling, intake, and care navigation.
Patient communication that patients respond to
Commure Engage brings these capabilities into one platform. It reaches patients across SMS, RCS, voice, and email, runs on 500+ clinically validated care pathways, and integrates bi-directionally with the EHR. More than 80% of patient inquiries resolve automatically, and outreach capacity scales up to 6.5x without adding staff.
What is patient communication software? Patient communication software is the platform a health system uses to reach and respond to patients across channels like text, voice, and email. Modern tools are two-way and AI-powered, so patients get answers and the care team stays in the loop, with everything connected to the EHR.
How is patient communication software different from an appointment reminder tool? A reminder tool sends one-way messages: appointment times, prep instructions, and alerts. Patient communication software adds a return path. Patients reply, get answers, and their responses route to the care team and into the EHR. The reminder becomes one feature inside a two-way system.
Is patient communication software the same as a patient portal? No. A portal waits for patients to log in. Patient communication software reaches patients on the channels they already use, like text and voice, and doesn't require a separate login or app.
Is texting patients HIPAA-compliant? It can be, with the right safeguards. Standard consumer texting isn't secure enough for protected health information. A HIPAA-compliant platform adds encryption, consent capture, access controls, and audit logging. The vendor also must sign a business associate agreement.
Who should own patient communication in a health system? It usually spans operations, IT, and clinical leadership, with input from marketing on voice and messaging standards. Operations owns the workflows, IT owns the EHR integration and security, and clinical teams shape the escalation and triage logic. Naming one accountable owner early keeps the program from fragmenting.
Hospitals lose about 3% to 5% of net revenue every year to revenue leakage, according to HFMA. Set that against the margin most systems actually operate on (the aggregate hospital operating margin is 5.2%), and the leak is roughly the size of the entire margin.
Most of that lost revenue gets chased after the fact. Retrospective chart audits, appeals on denied claims, quarterly reconciliation reviews. The work happens weeks or months after care was delivered, when the documentation has gone cold, and the filing window may already be closed.
Revenue integrity is the discipline built to stop that. It's the accuracy-and-compliance layer of the revenue cycle, and AI is moving it upstream: correctness enforced at the point of care, on every encounter, as it happens. That shift, from audit to assurance, is the story of this piece.
What is revenue integrity?
Revenue integrity is the practice of making sure what a health system documents, codes, and bills accurately reflects the care it actually delivered. The goal is to capture every dollar earned while staying compliant with payer and regulatory rules.
That means guarding accuracy in both directions. Under-capture costs you revenue you rightfully earned. Over-capture, like upcoding or billing for services that don't match the documentation, invites audits, recoupments, and compliance penalties.
In practice, healthcare revenue integrity spans several connected functions: clinical documentation, coding accuracy, charge capture, denial prevention, and underpayment recovery. A failure in any one of them surfaces downstream as lost or non-compliant revenue.
A revenue integrity function sits across clinical operations, coding, and billing, connecting teams that often work in silos. It ties the exam room to the balance sheet, which is where errors begin and where they get expensive.
Revenue integrity vs revenue cycle management
Revenue cycle management is the full pipeline: patient access, eligibility, charge capture, coding, claim submission, denials, and payment posting. It carries a service from delivery to payment.
Revenue integrity is the quality-control layer inside that pipeline. RCM asks whether a claim got paid. Revenue integrity asks whether it was right: coded to the correct level, supported by documentation, compliant, and complete.
You can run a fast revenue cycle that still leaks. Clean-looking claims get paid at the wrong amount, miss charges entirely, or trigger audits down the line. Revenue integrity is the check that keeps speed from turning into risk.
The documentation and coding accuracy pillar
Accurate reimbursement starts with accurate documentation. When a note fails to capture the full complexity of a visit, coders can't support the correct billing level, and the claim comes in low or wrong. The same gap distorts quality and risk-adjustment scores, since the codes that drive reimbursement also feed severity and outcomes reporting.
A service delivered but never charged never becomes a denial. It just disappears. That makes charge integrity the quietest form of revenue leakage and one of the hardest to catch.
Charges leak through lag, chargemaster mismatches, and manual processes that depend on someone remembering to enter a code. HFMA estimates as much as 1% of net charges are lost to charge integrity leakage, and its benchmarks call for capturing charges within 3 to 5 days and holding late charges under 2% of the total.
Denials are the visible symptom of upstream integrity failures. A denied claim usually points back to a documentation gap, a coding error, or an eligibility miss that happened well before the claim went out.
Commure customers using denial management tools with a pre-bill approach have cut pre-bill denials by 16% and reduced error rates by 35%, catching problems before claims are ever submitted.
How AI moves revenue integrity from audit to assurance
The traditional model is retrospective by design. Coders and revenue integrity teams review charts after discharge, auditors sample claims after payment, and appeals teams fight denials after the money's already been withheld. Each step catches some errors and misses others, and all of them cost time and staff.
AI changes the timing of that check, moving it to the moment care is delivered. During the visit, Ambient AI captures complete documentation while Autonomous Coding assigns accurate codes within seconds, each with its supporting rationale attached. On every encounter, Charge Note Reconciliation surfaces services that were documented but never billed, and denial tooling flags at-risk claims before they reach the payer.
Brought together on one platform, these steps make integrity continuous. Correctness gets built in as care is documented and coded, so fewer errors reach the claim and far fewer surface months later as denials or audit findings. It also means problems get caught while there's still time to fix them, before a filing window closes or a wrong claim goes out.
What a modern revenue integrity program looks like
A strong program is cross-functional by design, with clinical operations, coding, and billing sharing data and accountability across departments. It monitors continuously, flagging issues as they happen rather than collecting them for a quarterly cleanup.
Track the KPIs that expose leakage early: net collection rate (95% to 99% is the target), denial rate, charge lag, and avoidable write-offs held to 2% to 5% of net patient revenue, per HFMA. These numbers tell you where people, process, or technology are underperforming.
The technology layer, often called revenue integrity software, is what makes continuous checking practical at scale. The programs that get results treat revenue integrity as a revenue system in its own right, with the staffing, data, and executive attention that implies.
The bottom line
Revenue leakage runs about the size of a typical hospital's operating margin, and most of it still gets chased retrospectively. Revenue integrity closes that gap by keeping documentation, coding, and charges accurate from the start.
The move from audit to assurance is the real opportunity. AI makes correctness continuous, built into every encounter, so revenue integrity protects revenue in real time.
See how Commure RCM turns revenue integrity into a continuous process, from the exam room to the balance sheet.
Revenue leakage happens when care delivered doesn't fully convert into accurate, paid claims. The most common causes are incomplete clinical documentation, coding errors, missed or late charges, chargemaster mismatches, eligibility and authorization gaps, and denials that never get worked. HFMA estimates hospitals lose about 3% to 5% of net revenue to leakage each year, much of it invisible until a retrospective audit catches it.
What are revenue integrity KPIs?
Revenue integrity KPIs are the metrics that show where accuracy breaks down and revenue slips away. The core set includes net collection rate (95% to 99% is the target), initial and final denial rates, clean claim rate, first-pass rate, charge lag (capture within 3 to 5 days), late charges (under 2% of the total), and avoidable write-offs (held to 2% to 5% of net patient revenue). Tracking them continuously, rather than reviewing them quarterly, is what lets teams catch problems while there's still time to fix them.
Why is revenue integrity important in healthcare?
Revenue integrity matters because the money at risk is roughly the size of a hospital's entire operating margin. Hospitals lose an estimated 3% to 5% of net revenue to leakage each year, while aggregate operating margins run around 5.2% and close to 4 in 10 hospitals operate in the red. Getting documentation, coding, and charges right protects the revenue a health system earned and keeps it compliant, which guards against both lost income and payer audits.
Tell us a little bit about yourself - what do you like to do outside of work?
I'm happiest when I'm discovering something new. That curiosity has taken me through 10+ national parks, over 5 half marathons in different cities, and onto a snowboard for the first time this past winter. Exploring is my default mode, be it a new trail, a new neighborhood, or even a new country. When I'm not out adventuring, I'm mostly at a coffee shop with my lovely girlfriend or catching up with friends and family. I love long conversations that meander through every imaginable topic.
As a kid, what did you want to be when you grew up?
For a stretch, I was convinced I'd be an actor - I trained in drama and dance, and loved the idea of portraying different characters. While that dream faded, the instinct behind it continues to remain in that I love wearing different hats. As an engineer, that means moving between system design, team leadership, product strategy, and hands-on coding - sometimes all in the same day.
Describe a day in the life of your role.
No two days look the same, which is exactly how I like it. I usually start with mapping out my focus areas - whether that's writing a design document, reviewing PRs, shipping a feature, or sharpening one of my Claude skills for better accuracy.
Leading a team of four means regular syncs to stay aligned, but the most energizing moments are the unscripted ones: a cross-team whiteboard session on a tangled healthcare problem, or a breakthrough on something we'd been stuck on.
What made you decide to join Commure?
It was an unprecedented opportunity that turned out to be an excellent fit. Healthcare had always felt like meaningful territory to me, but I hadn't fully appreciated how transformative technology could be for the industry. Commure sits right at that intersection - where the mission is real and the technical challenges are genuinely hard. That combination was incredibly compelling.
How would you describe the Commure company culture?
Three focal points: ownership, speed, and versatility. People here own outcomes end-to-end, not just individual pieces of the work. We ship fast and iterate without ego. Everyone is encouraged to step outside their usual lane when solving problems that don’t fall neatly within their areas of expertise. It keeps things exciting.
What advice would you give someone on their first day at Commure?
On your first day at Commure, be curious and proactive. Ask questions early, seek feedback, and don’t wait for clarity to come to you. Talk to people whose work you admire - you’ll often learn more in one conversation than weeks of observation.
What has been your greatest accomplishment so far at Commure?
Leading the redesign of our Encounter Ingestion System - the pipeline that processes patient visit data at the core of our billing infrastructure.
As we scaled, the cracks in the old system became impossible to ignore: traceability gaps, duplicate encounters, tangled rule logic, operational blind spots. Instead of continuing to patch it, we tore it down and rebuilt it from first principles.
What we shipped was a platform built on three pillars: an Encounter Data Abstraction layer as a reliable source of truth for EHR data, the Genesis Rule Engine to unify transformations and validations in a flexible, scalable way, and end-to-end Auditability & Error Tracking so teams can see exactly how encounters are created - and exactly where things go wrong.
Watching that system roll into production and become the foundation for how we process encounters going forward is, without question, the work I'm most proud of at Commure.
Interested in a career building the next generation of healthcare technology powered by AI? We are always looking for talented people across our departments.
Ambient scribing gets most of the attention when clinicians talk about AI in the exam room. And for good reason, it's one of the most tangible, immediately impactful technologies to ever enter clinical practice. But there's a quieter, equally significant problem that AI is now starting to solve: what happens before a provider ever walks into the room.
Pre-charting. And for most clinicians, it's a significant, largely invisible drain on their day.
What Is Pre-Charting, and Why Does It Matter?
Before a provider sees a patient, the provider prepares by reviewing previous visit notes, checking recent labs, scanning the problem list, and looking through active medications. The goal is to walk into the encounter fully informed, understanding what's changed, what needs follow-up, and what the priorities are for this patient.
Done well, pre-charting enables better care. A physician who's done their homework before stepping into the room can be more present with the patient, ask more targeted questions, and make more confident clinical decisions. The preparation is the foundation for everything that follows.
The problem is that it takes time. A lot of it.
In a typical outpatient setting, pre-charting for even simple patient encounters can take 10 minutes or more. For a panel of 20 or 30 patients in a day, those minutes can compound into hours. In more complex care settings (oncology, for instance), pre-charting a single patient can take up to 30 minutes! Patients may have long and complex histories, extensive labs, imaging across multiple time points, and notes from multiple specialists. Getting up to speed on where a patient stands before a visit requires synthesizing an enormous amount of information scattered across a chart.
And just like documentation at the end of the day, pre-charting often spills outside of clinical hours. Physicians are doing it at home the night before and reviewing charts in the early morning before their first patient. The same "pajama time" problem that ambient scribing addresses on the documentation side exists on the pre-charting side too, it's just less visible, and less discussed.
The Limits of the EHR for Pre-Charting
Part of what makes pre-charting so time-consuming is the nature of the tools clinicians are using to do it.
Electronic health records were designed primarily as documentation and data storage systems. They were not built to synthesize clinical information on demand. A provider trying to quickly understand a patient's current clinical status has to navigate across multiple sections (notes, labs, imaging, problem lists, medications) and do the synthesis themselves. The EHR surfaces the data. The clinician does all the interpretive work.
This is a structurally inefficient workflow. It puts the burden of information aggregation on the clinician, whose strength is clinical judgment, not data retrieval. It's the same fundamental problem that makes documentation itself so burdensome: technology that forces providers to operate at the bottom of their license rather than the top.
What a Pre-Visit Summary Actually Does
A pre-visit summary is automated pre-charting. Rather than requiring a provider to navigate through a chart and assemble the clinical picture manually, the technology pulls together the relevant information and surfaces it in a structured, readable format.
Commure’s pre-visit summary functionality is made possible by our Patient360 platform, the clinical data foundation that makes AI useful at the point of care. Patient360 unifies a patient's full EHR history into a structured, queryable data object, surfacing specialty-tailored information, source-cited AI Q&A, and longitudinal patient context at the moment it matters most.
At its best, a pre-visit summary gives a provider (before they ever enter the room) a coherent view of:
Patient at a glance: why this patient is being seen, what makes them clinically distinctive, what the key active issues are
Last visit summary: what happened at the previous encounter, what was assessed and planned, what follow-up was ordered
Today's focus: relevant recent developments, outstanding labs or results, issues flagged for this visit
Active diagnoses and medications: current problem list and medication list in a reviewable format, including when medications were started
Social history and relevant context: information that shapes clinical decision-making but often takes time to locate in a standard chart view
This is the information a clinician is hunting for during pre-charting. A pre-visit summary delivers it in one place, automatically, before the visit begins.
The Hallucination Problem and Why It Has to Be Solved
Any clinician hearing about AI-generated clinical summaries has an immediate and legitimate concern: what if the system hallucinates a part of the history?
In clinical medicine, a hallucinated finding or fabricated lab result is a patient safety and medicolegal issue. A provider who sees inaccurate information in a pre-visit summary and relies on it in clinical decision-making is in a worse position than a provider who had to do pre-charting manually.
This is why any serious pre-visit summary technology has to solve the attribution problem, not just the synthesis problem. It's not enough to generate a summary that reads well. Every clinical claim in that summary needs to be traceable to a specific source in the patient's chart so the provider can verify the information, understand its provenance, and calibrate their confidence accordingly.
Expandable citations that link directly to the source documentation (the specific note, the specific lab result, and the specific imaging report) are what make pre-visit summaries trustworthy. The AI does the synthesis. The clinician retains the ability to verify.
Turning Pre-Visit Summaries Into Clinical Intelligence
For patients with complex, longitudinal histories (chronic illness, oncology, or multi-system disease to name a few), even a well-constructed summary may leave questions unanswered. A provider might want to know what happened to a specific lab value over the past year, or which specialist last addressed a particular issue, or whether a medication change in the last visit was associated with any documented side effects.
When a pre-visit summary is built on top of a comprehensive patient data framework, providers can ask those questions directly. Natural language queries against the patient's chart, surfacing abnormal labs since the last visit, flagging documented changes in condition, and answering specific clinical questions. All of this becomes possible without leaving the workflow.
This is a meaningful shift in how providers interact with clinical information. Instead of navigating a chart and hoping they don't miss something, they can ask specific questions and get specific answers, with the underlying documentation available for review.
Connecting Pre-Visit Preparation to Documentation
Pre-visit summaries and ambient documentation aren't separate products with separate value propositions. They're two components of a continuous clinical workflow, one that starts before the patient arrives and ends with a complete note after they leave.
A provider who has reviewed an AI-generated pre-visit summary before the encounter walks in prepared, already thinking about the clinical priorities for this visit. When the encounter begins, and ambient documentation starts capturing the conversation, the provider is already operating at a higher level, asking better questions, engaging more directly with the patient's concerns, and making more informed decisions in real time.
The downstream effect is documentation quality. The clinical picture that the ambient AI captures is richer because the encounter itself was richer. Diagnoses are more specific. The assessment and plan reflect more precise clinical reasoning. Coding suggestions that emerge from the documentation are more accurate because the documentation more faithfully reflects the complexity of the care that was actually delivered.
What This Means for Providers
The conversation about AI in healthcare has spent a lot of time on what AI can do after the clinical encounter (documentation, coding, billing). But it represents only part of the opportunity.
The administrative and cognitive burden on physicians doesn't begin when the visit ends. It begins when the workday starts. Pre-charting is where providers spend time that they can't easily account for, that doesn't show up in RVU counts, and that no one has historically built technology to address.
Pre-visit summaries change that. They return time to providers at the front of the clinical day, not just the back. They reduce the cognitive load that accumulates before a provider has even greeted their first patient. And they create the conditions for a better clinical encounter, which is ultimately what both providers and patients are there for.
The technology to automate this work exists now. Providers who are already experiencing two hours of pajama time at the end of the day shouldn't also be spending significant time on manual pre-charting at the start of it. That's a problem with a solution, and AI is ready to deliver it.
Interested in learning more about how Commure's Patient360 platform and pre-visit summaries can work for your organization? Contact Dr. Jean-Luc Neptune, Clinical Commercial Leader at Commure, at jeanluc.neptune@commure.com.
What makes charge capture errors so dangerous is that they never show up as a denial. There's no rejection to appeal, no error message, no line on a dashboard. The charge simply never gets created, and by the time anyone notices, the timely filing windows have closed.
So before you tune your denials process or renegotiate a payer contract, look at the part of the revenue cycle where the leakage actually starts.
What charge capture is
Charge capture is the process of recording every billable service, supply, and procedure from a patient encounter so it can be coded and billed.
It happens at or right after the point of care, during charting, or immediately after the patient leaves. It's the handoff between the care a clinician delivers and the claim your billing team builds.
Two distinctions matter. Charge capture and coding are separate steps: coding translates the captured service into CPT and ICD-10 codes after the charge exists. Charge capture also depends on clinical documentation. If a service isn't documented, it usually won't be charged, meaning it won't be coded, billed, or paid.
Why revenue leaks at the charge
Charge capture breaks in quiet ways.
A clinician finishes a procedure and moves to the next patient before the charge is entered. An incision is made and an implant is placed in the OR, but no corresponding charge is recorded. An E&M visit gets documented at a lower complexity than the care actually delivered. Supplies used at the bedside never make it onto the bill.
Each miss is small. Across thousands of encounters a month, the small misses compound into real money.
Charge lag adds to the problem. The longer the gap between the service and the charge, the more detail gets forgotten, and the closer the claim drifts toward its filing deadline. Chargemaster mismatches make it worse: clinical practice changes faster than the codes and pricing logic behind it, so the charge that does get recorded may not reflect the full value of what was delivered.
The root cause is usually a manual process. When charge entry depends on memory, spreadsheets, and retrospective chart review, coverage is thin and slow. Most manual reconciliation touches a fraction of charts, and it happens after claims have already gone out.
To make things worse, these missed charges are permanent. You can rework a denied claim. You cannot bill for a service you never recorded once the filing deadline passes.
Hospital charge capture is harder at scale
The bigger the organization, the more places a charge can fall through.
Hospitals bill both facility and professional fees, and the two don't always line up. High-volume, high-acuity settings like the emergency department make real-time capture difficult because clinicians are focused on patients, not charge tickets.
Procedure-heavy specialties carry the most risk. Cardiology, orthopedics, radiology, and surgical services all involve dense documentation and high-dollar items that are easy to miss or undercount.
When charge capture depends on people remembering to act, every open seat on a revenue cycle team is a gap in coverage.
Eligibility, coding, claim submission, denials, and posting all depend on a charge existing in the first place. A clean claims rate can look healthy right up until you realize it can't recover a charge that was never created.
This is why charge capture deserves attention as a strategic control. It's the first point where clinical activity turns into revenue, and the one point where a loss can't be recovered.
How AI is changing charge capture software
For years, charge capture software meant a mobile app that let clinicians enter charges faster. Useful, but still dependent on a human remembering to enter the charge.
AI changes the model. Rather than waiting for someone to log a charge, the system reads the clinical note, compares what was documented against what was billed, and flags services that were documented but never charged.
This is the difference between charge capture and charge note reconciliation. Charge capture depends on someone remembering to act. Charge note reconciliation runs automatically on every encounter, whether or not anyone did.
That shift in coverage is the whole point. Manual review samples a slice of charts after the fact; automated reconciliation reads all of them before the claim goes out, which is when a missed charge can still be fixed.
Pair that with autonomous coding, which generates CPT and ICD-10 codes directly from the documentation, and the path from encounter to clean claim gets shorter and more accurate. The same approach turns charge capture solutions from a faster way to type into a safety net that runs automatically.
What this looks like in practice
The proof is in what happens when health systems close the gap.
HFMA documented Novant Health, a 14-hospital system with $4.3 billion in net patient revenue, that uncovered $7.5 million in recoverable revenue within 15 months of overhauling its charge capture process. That was revenue from services that had been delivered, documented, and then missed.
Commure built charge capture and charge note reconciliation into Commure Pro, the clinical intelligence platform clinicians use at the point of care, and connected it to the broader RCM platform so a captured charge flows straight toward the claim.
Charge capture is the front end of getting paid for care you've already delivered.
When it runs on memory and retrospective review, revenue leaks quietly and permanently. When the clinical note, the charge, and the code connect automatically, the leak closes and the revenue shows up where it should.
If you're rethinking where your revenue cycle loses money, start at the charge. It's the cheapest dollar to recover, because it's a dollar you already earned.
See how Commure connects charge capture to the rest of the revenue cycle.








.jpg)



.jpg)
.jpg)


