





Best AI Medical Scribes 2026: Top 10 Tools Compared
A methodology-first comparison of ten AI medical scribes, built on KLAS scores, published studies, and sourced pricing rather than vendor claims.

Medically Reviewed by Dr. Jean-Luc "JL" Neptune, Clinical Commercial Leader
Written by the Commure Scribe Team
Published: March 3, 2026
•
16 min read
Updated July 31, 2026
What You Need to Know About the Best AI Medical Scribe Tools
- The best AI medical scribe is the one that reduces a clinician's workload, whether that's note-taking or clicks.
- A scribe built for primary care won't necessarily work for oncology, and one built for Epic won't necessarily work for athenahealth. Specialty and EHR both change what fits.
- KLAS scores, published studies, and other verifiable facts separate one scribe from another.
- Published pricing and free trials let you decide faster, on your own schedule.
How Do the Top 10 AI Medical Scribes Compare?
Commure Scribe is one of the ten products compared here, and we've ranked it #1. We scored it against the same criteria as every other product below. See our methodology so you can judge for yourself.
The clearest divide among these ten tools is sales model, not features: four publish pricing and offer self-serve signup, the other six sell through enterprise teams and keep pricing private. For those six, the table uses third-party estimates, sourced and noted as such.
Only three of the ten have a published third-party performance score: DeepScribe (98.8), Abridge (95.3), and Commure Scribe (93.3). The other seven. Freed, Nabla, Heidi Health, DAX Copilot, Suki, Sunoh.ai, Ambience, don't disclose independent validation.
Confirm current pricing directly with each vendor before contracting. Enterprise vendors typically add setup, IT, and training costs on top of the monthly rate.
What Are the 10 Best AI Medical Scribes in 2026?
The best AI medical scribe pick depends on which criteria matter most to your team. The ten profiles below apply the same six to each tool: third-party proof, pricing, trial access, EHR fit, coding support, and setup time.
Competitor figures come from each vendor's own site or a named third party. Treat them as vendor-reported unless a study is cited.
1. Commure Scribe
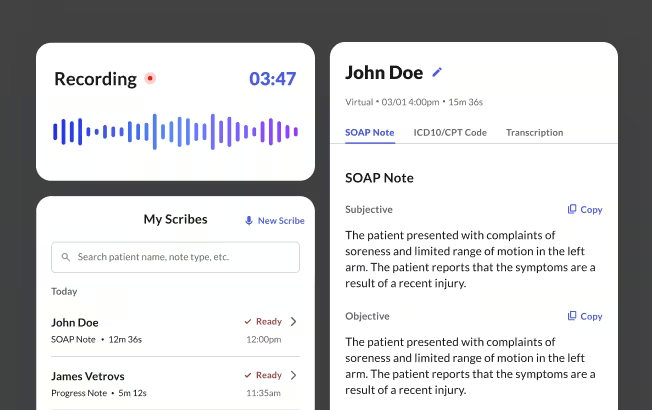
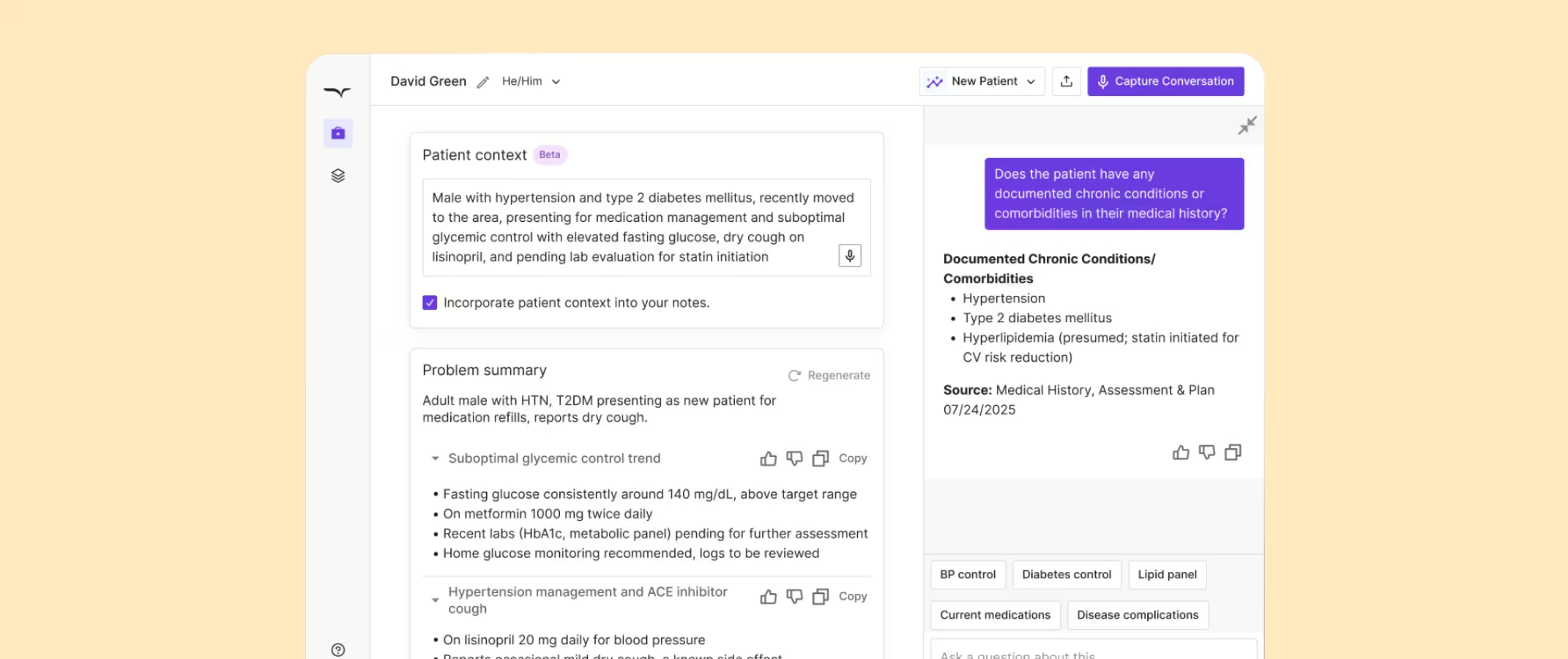
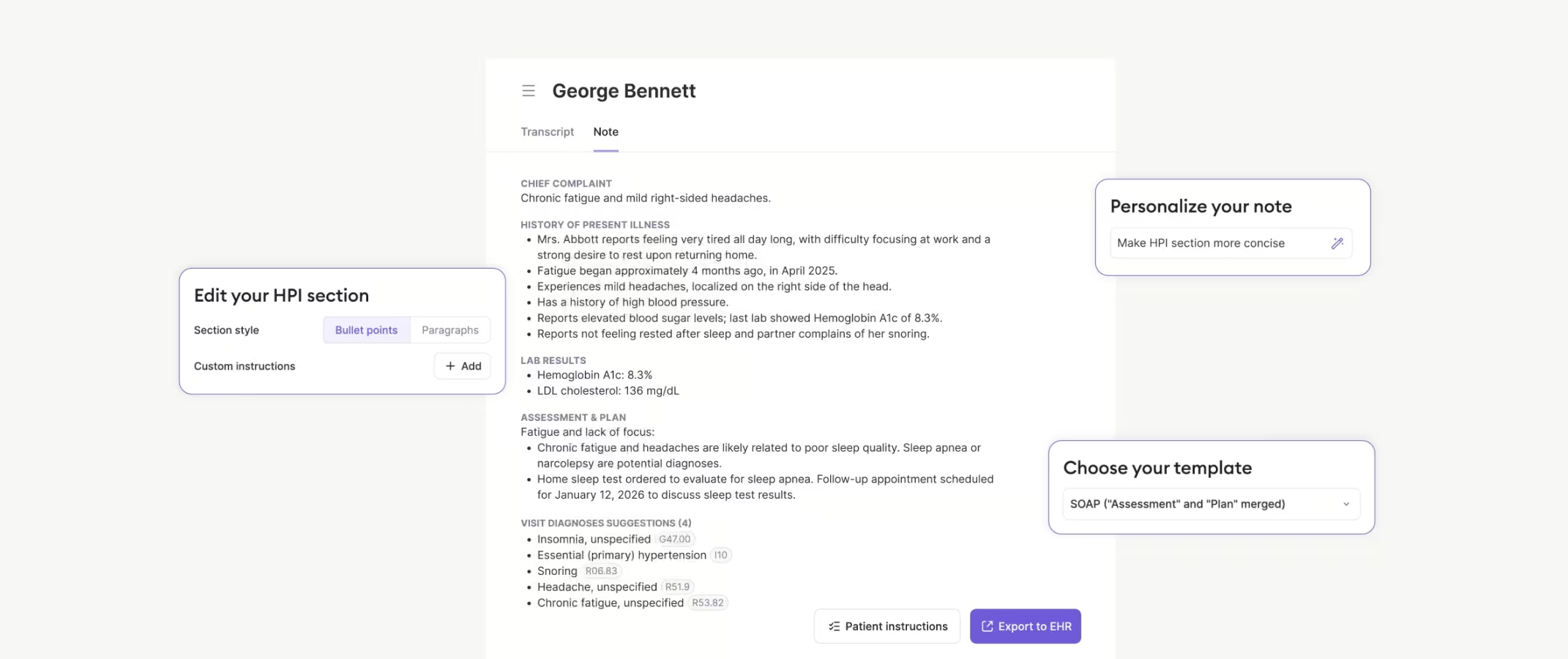
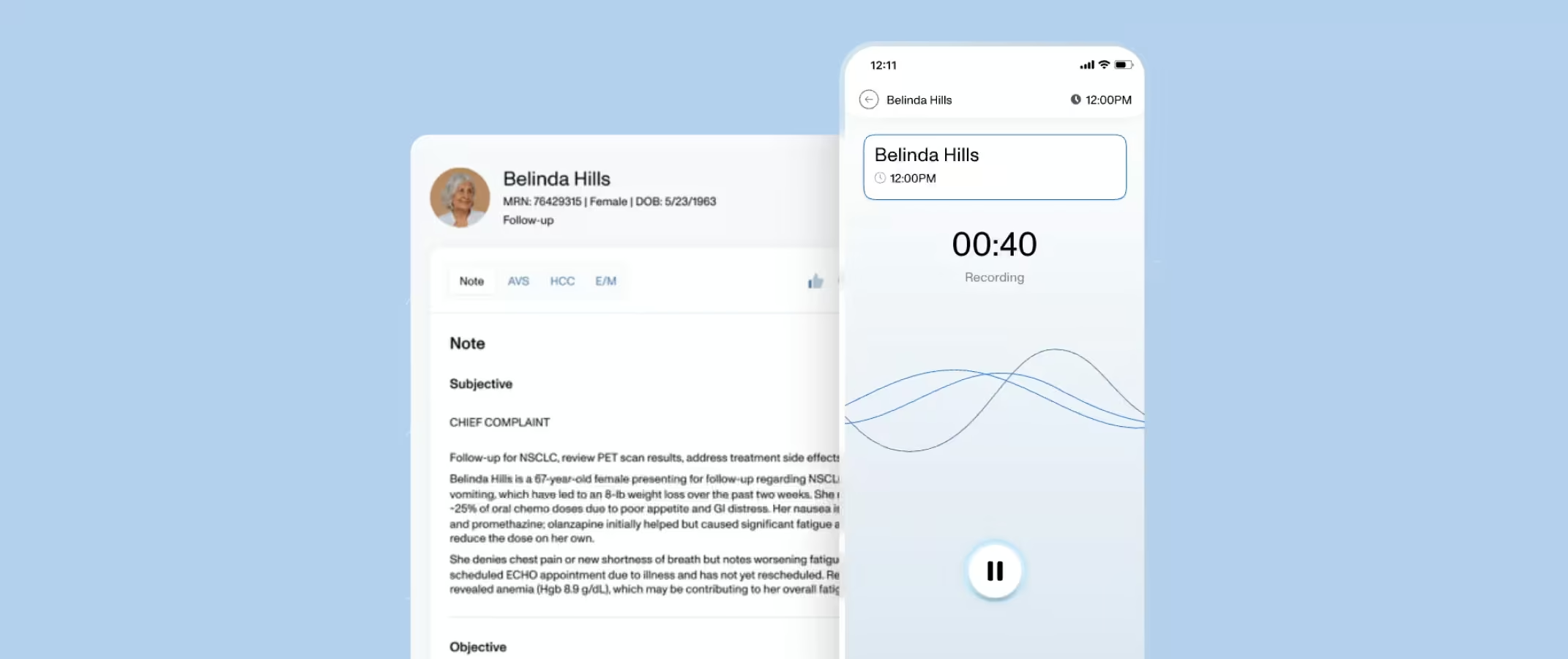
Commure Scribe is an ambient AI medical scribe used by 75,000+ clinicians across 25M+ patient encounters annually. The workflow is Capture, Edit, Finalize, and the clinician always has the option to review before finalizing. It supports 90 languages with automatic detection and records up to 2 hours per session.
It works on any device for in-person and telehealth visits. It generates suggested ICD-10 and CPT codes at the entry price and offers 60+ EHR integrations, including athenahealth, eClinicalWorks, and AdvancedMD. One-click EHR sync, custom AI workflows, and ROI analytics are group-plan features; solo and small practices use copy-paste for EHR handoff. 90%+ of providers reduce clinical documentation time and digital fatigue.
Commure's ambient AI platform earned 93.3 in a 2025 KLAS First Look²⁴.
Pricing: starts at $89/mo for solo and small practices. A 7-day trial requires no credit card. For current rates and plan details, see the Commure Scribe pricing guide.
Best for: Solo clinicians and group practices that need coding andnative EHR sync built into the workflow, whatever the practice size.
2. Freed
Freed is a self-serve AI medical scribe built for solo and independent clinicians. The vendor reports 20,000+ clinicians across 1,000+ health organizations⁸. It supports 90+ languages with automatic detection and adaptive templates that learn from clinician edits⁸. Audio is deleted automatically after note generation, typically within 60 seconds²³.
Setup runs through a 15-minute self-serve wizard⁸. EHR push is a Premier-tier Chrome extension with no bidirectional sync. Coding support is available on the $119/mo Premier tier only. The vendor states the product is designed for independent clinicians rather than large health systems⁸.
Pricing: $39/mo Starter (40 notes), $79/mo Core (unlimited), $119/mo Premier⁸. The 7-day trial needs no credit card⁸.
Best for: Solo clinicians who want the lowest entry price and are willing to handle coding separately or upgrade to Premier for it.
3. Nabla
Nabla is an ambient AI medical scribe deployed at 130+ organizations, per the vendor⁹. In the field's first randomized controlled trial, Nabla cut physician time-in-note by 9.5% versus control⁵. Its Nabla Connect module embeds in the EHR, pulls patient history in, and pushes notes back⁹.
Audio is processed in chunks and discarded⁹. Notes default to a 14-day configurable retention window⁹. Nabla holds SOC 2 Type II and ISO 27001 certifications⁹. A free tier with volume limits is available with no expiry. ICD-10 and CPT coding are not yet available; the vendor says they are in development⁹.
Pricing: Nabla offers a free and paid tier structure but does not publish paid pricing⁹.
Best for: Practices wanting a no-expiry free tier to test ambient scribing before committing; not yet a fit if coding support is required.
4. DeepScribe
DeepScribe is an enterprise AI medical scribe with bidirectional integrations for Epic, Athenahealth, and eClinicalWorks¹⁰. Its Clinical Moments feature lets a clinician highlight note text and trace it to the source moment in the conversation¹⁰, supporting note-to-conversation auditability for medico-legal review. It supports ICD-10, HCC, and CPT coding.
In 2025, DeepScribe earned a 98.8 performance score from KLAS Research¹⁰. Audio retention is not disclosed in detail; the privacy policy states data is kept as long as necessary for the identified purpose²⁰. There is no self-serve trial.
Pricing: custom. Not published; confirm with vendor.
Best for: Large health systems that need bidirectional Epic,
athenahealth, or eClinicalWorks sync and note-to-conversation
auditability for medico-legal review.
5. Heidi Health
Heidi Health lists Beth Israel Lahey Health as a named US customer¹². The vendor reports 2.4 million consults per week and 110 languages¹². It lists 20 named EHR integrations, including Epic Hyperspace via SMART on FHIR and athenahealth¹². Audio is never stored; it is transcribed in real time and immediately discarded²¹. ICD-10 and CPT coding are available on the Enterprise tier only; free and mid-tier plans do not include coding¹².
Pricing: a permanent $0 free tier with unlimited AI notes, then $30 to $180 per user per month across paid tiers, billed annually¹². Enterprise tier pricing is custom and not published. Paid tiers carry a 14-day trial¹².
Best for: Individual clinicians who want a permanent free tier to trial AI scribing before paying; coding and EHR write-back require upgradingto Enterprise/Practice tiers.
6. Nuance DAX Copilot
DAX Copilot is Microsoft's ambient AI medical scribe, sold to enterprise health systems with a native Epic embed and Microsoft Azure infrastructure¹³. It is a separate product from the dictation-first Dragon Medical One, covered in this Nuance Dragon Medical One review. It holds HITRUST CSF certification through the Nuance cloud¹³.
It captures English and, per Microsoft's support documentation, Spanish in the US with a manual pre-visit toggle¹³. Notes generate in English regardless of visit language¹³. In the UCLA randomized trial, DAX showed no statistically significant change in physician time-in-note⁵.
Pricing: enterprise sales only. Not published; confirm with vendor.
Best for: Epic health systems already standardized on Microsoft/Nuance
infrastructure and set up for a custom enterprise sales process.
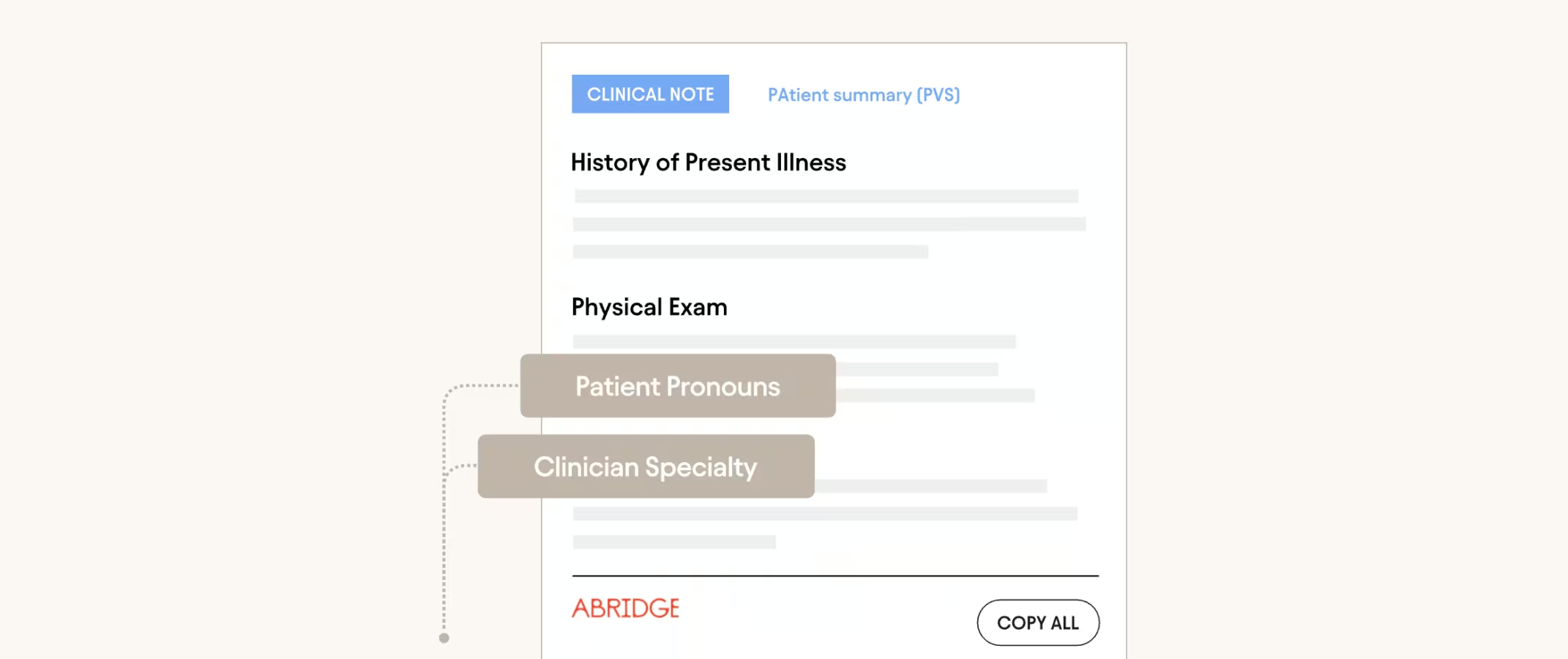
7. Abridge
Abridge is an enterprise AI medical scribe deployed across 150+ health systems, including Mayo Clinic, Johns Hopkins, and UPMC¹⁴. The vendor reports 1M+ conversations weekly¹⁴. Each note sentence links back to the transcript or audio so clinicians can check the source¹⁴.
Abridge holds a 95.3 KLAS score, per its KLAS page²⁵. It is Epic-first; smaller groups access it mainly through an athenahealth partnership.
Pricing: enterprise sales only. Not published.
Best for: Epic-integrated health systems that want source-linked notes for audit.
8. Suki
Suki is an enterprise AI medical scribe and assistant that pairs ambient notes with voice control of the EHR¹⁵. Clinicians can pull patient data, stage orders, and ask clinical questions by voice¹⁵. Each note sentence is grounded in the EHR or transcript. It supports ICD-10, CPT, HCC, and E/M coding. Audio and transcripts are permanently deleted after 30 days²².
It supports 80+ languages with automatic detection and 100+ specialties per the vendor¹⁵. Bidirectional integrations cover Epic, Oracle Health, athenahealth, and MEDITECH¹⁵. Sold through enterprise sales only; there is no self-serve option.
Pricing: custom. Not published; confirm with vendor.
Best for: Large health systems wanting voice-controlled EHR actions (pulling data, staging orders) bundled with ambient notes.

9. Sunoh.ai
Sunoh.ai is an AI medical scribe integrated into the eClinicalWorks ecosystem¹⁶. It offers an ambient scribe workflow for eCW users. No KLAS score or published study surfaced in this evaluation. Organizations not on eClinicalWorks should confirm integration support with the vendor.
Pricing: check with the vendor. No published figure met this article's sourcing standard.
Best for: Practices fully standardized on eClinicalWorks with no other EHR requirements.
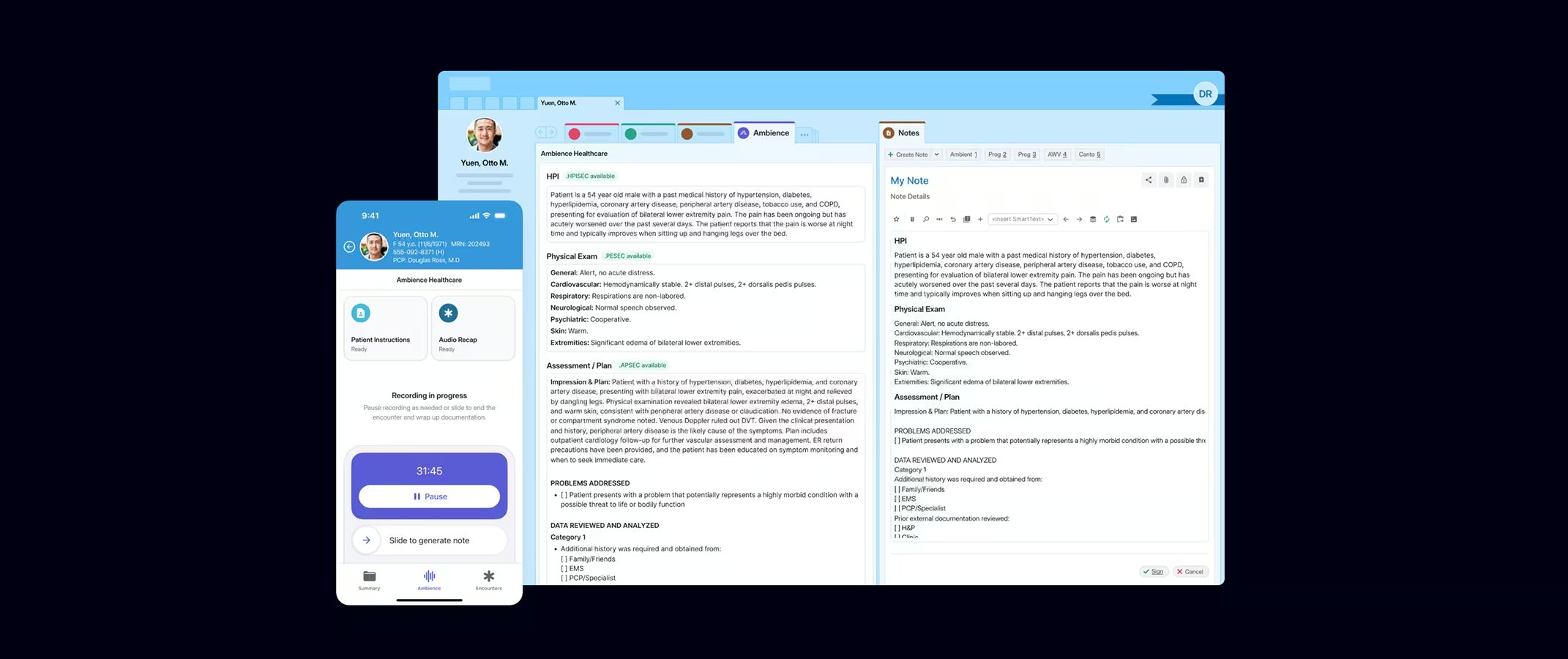
10. Ambience
Ambience is an enterprise AI medical scribe platform focused on HCC and E/M coding accuracy for organizations with risk-adjusted contracts.
A KLAS Research study commissioned by Ambience examined a St. Luke's Health System deployment¹⁷. It reported $13,000 per clinician per year from improved HCC and E/M coding¹⁷, a 41% cut in chart closure time, and 22% more patient face time¹⁷.
Pricing: custom enterprise pricing; no published figures.
Best for: Health systems on risk-adjusted contracts prioritizing HCC andE/M coding accuracy over self-serve trial access.
How Were These AI Medical Scribes Evaluated?
We scored every product on this list against six criteria.
- Is there independent evidence behind it? We weighted KLAS Research scores, published studies, and peer-reviewed data over anything a vendor says about its own product.
- Does it write directly into the EHR, or do you have to copy-paste? Native integration counts for more, and so does how many EHR systems it covers.
- Is the price posted, or do you have to talk to sales to find out?
- How much stands between signing up and actually trying it? A free trial with no credit card scores higher than one gated behind a sales call.
- How long does it take to go from signup to actually using it with patients?
- Does it suggest ICD-10 and CPT codes, and is that a validated capability or just a feature name?
Validation and EHR integration count for the most. Those are the two things that actually hold up once a tool leaves the demo and gets used in a real clinic. Commure Scribe went through the same six checks as everything else on this list.
What Do Physicians Say About AI Scribes in Practice?
Physician-reported experience with AI medical scribes is more nuanced than vendor marketing suggests. No verified discussion threads met this article's sourcing standard, so this section draws on published physician surveys instead. The same themes recur across them: praise for presence and pace, complaints about errors and editing.
What physicians praise:
- Patient connection. In Permanente surveys, 84% of physicians said the technology improved patient interactions. Another 82% reported better work satisfaction¹⁹.
- Patients notice too. In the same surveys, 47% of patients said their doctor spent less time on the computer¹⁹.
- Low patient pushback. In the UCLA trial, physicians estimated about 7% of patients declined the AI scribe⁵.
What physicians complain about:
- Omissions, not fabrications. UCLA trial physicians reported omissions as the most common error type, ahead of structural issues and pronoun mix-ups⁵.
- Editing time. Inaccuracies were rated as occurring "occasionally," which still means review work on most notes⁵.
- Abandonment. About 15% of trial physicians never used their assigned scribe during the two-month study⁵.
The pattern carries a buying lesson. Physicians who fold review into their workflow report the gains. Physicians who expect a hands-off AI medical scribe drift back to manual charting.
The UCLA authors put it plainly: ongoing physician oversight is needed to keep notes faithful to the visit⁵.
Why Are Clinicians Moving to AI Medical Scribes in 2026?
AI medical scribe adoption is rising because the charting burden has not eased even as burnout has. In 2023, 48.2% of US physicians reported at least one burnout symptom, down from 53%¹. Yet 20.9% still spent over eight hours per week in the EHR after hours, unchanged year over year¹.
Physicians spend up to two hours on EHR work per hour of direct patient care².
The evidence base has also matured. A 2026 JAMA cohort followed 8,581 clinicians at five academic medical centers³. AI medical scribe adopters cut charting time by 16 minutes per eight scheduled patient hours³.
Roughly 30% of US physician practices now use some form of AI medical scribe⁴.
That maturity raises the bar for picking the best AI medical scribe for a given setting. The market spans low-cost self-serve apps and enterprise platforms sold through long sales cycles. Pricing, trial access, EHR fit, and coding support vary widely across the ten AI medical scribes compared here.
How Much Does an AI Medical Scribe Cost?
Published self-serve AI medical scribe pricing runs from $39 to $119 per clinician per month, based on the vendor pages cited above. Enterprise AI medical scribes cost several times more, and most keep pricing private.
Three cost layers matter beyond the subscription line:
- Tier gating. Several vendors place coding, EHR push, or analytics on higher tiers. Price the tier that has the features you need, not the advertised entry price.
- Setup and support. Enterprise deployments add IT work, security review, and training. Ask each vendor to itemize these costs before signing.
- Contract structure. Annual billing discounts are common, but they lock in a tool before a care team knows whether it sticks.
The revenue side can offset part of the cost. A UCSF study of 1,565 physicians found adopters generated 1.81 more RVUs per week²⁰.
That 5.8% gain is worth about $3,044 per physician per year at 2025 Medicare rates²⁰. Claim denials did not rise²⁰.
The study authors noted the gains may partly reflect changed coding practices rather than pure productivity²⁰.
Independent reviewers still urge caution on the full ROI math. The Peterson Health Technology Institute reports that health system leaders see the financial impact of AI medical scribes as unclear once all costs are counted⁶.
How Do You Choose the Right AI Scribe?
The best AI medical scribe for your team is the one that survives a structured trial. Match the shortlist to your sales-model tolerance first.
A solo clinician can test three self-serve AI medical scribes in a month at little or no cost. A large group choosing an enterprise AI medical scribe should demand a pilot cohort before an org-wide contract.
Design the trial around real use, not demos:
- Test on your hardest encounters. Multi-speaker visits, interpreter visits, and complex histories expose weaknesses that a demo hides.
- Score the edit time, not just the draft. Track how long each note takes from recording stop to signature across the trial.
- Check the EHR path end to end. Confirm how notes move and on which tier. Copy and paste, browser extension, and true sync behave differently.
- Check coding output against your billing workflow. Suggested codes help most when coders review them as usual.
Two AI medical scribe adoption findings from large deployments should shape the rollout plan. In the Permanente deployment of 7,260 physicians, heavy users saved 2.5 times more time per note than occasional users¹⁹. The same analysis found no link between physician age and adoption¹⁹.
Users averaged about 47 years old¹⁹. Consistent use drives the benefit, and seniority is not a barrier.
Specialty fit deserves a direct question rather than a brochure answer. Ask each vendor which templates exist for your specialty today and which need custom builds. Then confirm the answer inside the trial with your own visit types.
Specialty-specific shortlists can help here. See the guides to the best AI scribe for family medicine and the best AI scribe for psychiatry. Pediatric teams have a dedicated best AI scribe for pediatrics guide.
If no AI medical scribe earns trust during trials, weigh alternatives to AI medical scribes. Human scribes and dictation beat a default back to manual charting.
How Does Commure Scribe Fit a Best AI Medical Scribe Shortlist?
Commure Scribe maps to the six criteria this comparison applied. The Capture, Edit, Finalize workflow keeps the clinician in the loop, with the option to review before finalizing. Per internal survey data, 90%+ of providers reduce clinical documentation time and digital fatigue, and clinicians report a 43-second average chart close time.
Pricing is published. For current rates and plan details, see the Commure Scribe pricing guide.
The platform is EHR-agnostic, with 60+ EHR integrations, which matters for organizations that do not run Epic. Solo and small practices use copy and paste; medium and large groups get one-click sync.
The 7-day unlimited trial needs no credit card, so a care team can try Commure Scribe on real encounters before any contract. Larger groups scoping a structured pilot can book a Commure Scribe demo.
This article is for informational and educational purposes only, does not constitute legal, medical, or professional advice, and does not guarantee any particular pricing, performance, or purchasing outcome.
Frequently Asked Questions
Many AI medical scribes do, through different paths. Abridge, DAX Copilot, DeepScribe, Suki, Nabla, and Heidi list Epic integrations, while Suki also lists Oracle Health (Cerner) and MEDITECH. Other tools rely on copy and paste or browser extensions. Confirm the integration method and tier for your specific EHR version before buying.
No independent head-to-head benchmark names the best AI medical scribe for accuracy across vendors. The strongest third-party signals are KLAS scores: DeepScribe leads at 98.8 and Abridge follows at 95.3. Commure's ambient AI platform holds at 93.3, all from 2025 KLAS reporting. The UCLA randomized trial is the other major signal; in that trial, physicians reported omissions as the most common error type, so clinician review remains essential with any tool.
Self-serve AI medical scribes usually run month to month, with discounts for annual billing. Enterprise platforms typically need annual or multi-year agreements negotiated through sales.Before committing, use trial periods. Several tools offer 7-day trials, while Heidi Health and Nabla offer free tiers without expiry.
Most leading AI medical scribes state HIPAA compliance and sign business associate agreements, but the details differ by vendor. Audio storage, retention periods, and AI training policies vary widely. Ask each vendor for its BAA, its audio retention policy, and its security certifications such as SOC 2 before contracting.
Published self-serve pricing runs from $39 to $119 per clinician per month across AI medical scribes like Freed, Commure Scribe, and Heidi Health. Enterprise platforms use custom quotes and do not publish pricing. Setup fees, training, and IT work add to enterprise totals.
Some AI medical scribes can, and tier placement matters. Commure Scribe includes suggested ICD-10 and CPT codes at its entry price. Suki and DeepScribe add HCC and E/M support.Freed gates coding to its Premier tier, Heidi to its Enterprise tier, and Nabla has no coding yet. Codes are suggestions for clinician and coder review, not automated billing.
Sources
- American Medical Association, "Burnout on the way down, but 'pajama time' stands still," https://www.ama-assn.org/practice-management/physician-health/burnout-way-down-pajama-time-stands-still, 2024.
- UCLA Health, "UCLA study finds AI scribes may reduce documentation time," https://www.uclahealth.org/news/release/ucla-study-finds-ai-scribes-may-reduce-documentation-time, 2025.
- Rotenstein, Holmgren, Thombley, et al., "Changes in Clinician Time Expenditure and Visit Quantity With Adoption of Artificial Intelligence–Powered Scribes," JAMA, https://jamanetwork.com/journals/jama/article-abstract/2847319, 2026.
- Columbia University School of Nursing, "Health Care's Rush to AI Scribes Risks Patient Safety," https://www.nursing.columbia.edu/news/health-cares-rush-ai-scribes-risks-patient-safety-researchers-warn, 2025.
- Lukac et al., "Ambient AI Scribes in Clinical Practice: A Randomized Trial," NEJM AI, https://pmc.ncbi.nlm.nih.gov/articles/PMC12768499/, 2025.
- Peterson Health Technology Institute, "Leading Health Systems: AI-Powered Scribes Alleviate Clinician Burnout," https://phti.org/announcement/ai-scribes-reduce-clinician-burnout/, 2025.
- Freed, "Pricing," https://www.getfreed.ai/pricing, 2026.
- Nabla, "EHR Integrations," https://www.nabla.com/ehr, 2026.
- DeepScribe, "Trust Center Updates," https://trust.deepscribe.ai/updates, 2025.
- Heidi Health, "Pricing," https://www.heidihealth.com/en-us/pricing, 2026.
- Nuance (Microsoft), "DAX Copilot," https://www.nuance.com/healthcare/dragon-ai-clinical-solutions/dax-copilot.html, 2026.
- Abridge, "Trust Center," https://trust.abridge.com, 2026.
- Suki, "Suki Assistant," https://www.suki.ai/suki-assistant, 2026.
- eClinicalWorks, https://www.eclinicalworks.com, 2026.
- Ambience Healthcare, "KLAS Ambient AI Scribe ROI Validations," https://www.ambiencehealthcare.com/resources/klas-ambient-ai-scribe-roi-validations, 2025.
- npj Digital Medicine, "Policy brief: ambient AI scribes and the coding arms race," https://www.nature.com/articles/s41746-025-02272-z, 2025.
- DeepScribe, Privacy Policy, 2026. https://www.deepscribe.ai/privacy
- Heidi Health, "Data & Security at Heidi Health," 2026. https://www.heidihealth.com/support/en/articles/8885107-data-security-at-heidi-health
- Suki AI, Security & Compliance FAQ, 2026. https://developer.suki.ai/documentation/faqs/security
- Freed, "How Freed Protects Patient Data and Ensures Compliance," 2026. https://www.getfreed.ai/blog/how-freed-handles-data-privacy-compliance
- The Permanente Medical Group, "Analysis: AI scribes save physicians time, improve patient interactions," https://permanente.org/analysis-ai-scribes-save-physicians-time-improve-patient-interactions-and-work-satisfaction/, 2025.
- UCSF, "UCSF Study Finds AI Scribes Associated with Increased Physician Productivity and Revenue," https://docit.ucsf.edu/news/ucsf-study-finds-ai-scribes-associated-increased-physician-productivity-and-revenue, 2025.
- Commure, "Commure Ambient AI Scores High Marks in KLAS First Look Report," https://www.commure.com/press-releases/commure-ambient-ai-scores-high-marks-in-klas-first-look-report-for-automating-provider-documentation-rcm, 2025.
- Abridge, "Abridge wins Best in KLAS for the Ambient AI segment," https://www.abridge.com/best-in-klas, 2025.



.jpeg)