




AI in Primary Care: A Guide for Independent and Group Practices
What documentation, decision support, inbox, chronic disease, and prior authorization AI tools do and how to start without an IT team.
Written by the Commure Scribe Team
Published: April 17, 2026
•
9 min read
Updated June 26, 2026
AI use in primary care doubled in a single year. The AMA’s 2024 survey found 66% of physicians using some form of healthcare AI, up from 38% in 20233, a rate the AMA described as “unusually fast.” The tools span five categories: documentation, clinical decision support, patient inbox management, chronic disease management, and prior authorization. This guide covers what each category does, what the evidence shows, and where independent and group practices should start.
What You Need to Know
- Nearly two-thirds of physicians reported using healthcare AI in 2024, up from 38% in 2023. Adoption is uneven: documentation tools have the widest deployment, while clinical decision support and inbox AI remain early-stage in most independent practices.³
- About 5% of US outpatient patients experience a diagnostic error annually, with 33% of those leading to permanent severe injury or death.⁷ Real-world evidence for AI decision support tools in primary care settings is still limited.
- Burnout dropped from 51.9% to 38.8% after 30 days of ambient scribe use across six health systems.⁴
What does AI in primary care cover?
AI in primary care spans five tool categories: documentation, clinical decision support, patient inbox management, chronic disease management, and prior authorization. Each targets a different part of the clinical day and has a different evidence base, deployment profile, and setup requirement for independent and group practices.
Why is AI in primary care getting attention now?
The AMA’s 2024 Augmented Intelligence Research Survey found that 66% of physicians reported using healthcare AI, up from 38% in 2023.3 The survey found documentation and administrative burden as the top drivers: 57% of physicians identified reducing administrative burdens through automation as the biggest area of opportunity for AI in their practice.
For independent and group practices, there is no IT team to manage rollout and no clinical informatics staff to monitor performance. Tools need to work with existing hardware and show value within the first few visits.
What are the main categories of AI in primary care?
Documentation
Ambient documentation tools record the clinical encounter and generate a structured note for the clinician to review and finish. Primary care physicians spend as much as two hours on EHR documentation for every one hour of direct patient care,1 and 20.9% of physicians spent more than eight hours per week on EHR work outside normal hours in 2023, unchanged year over year.2 Ambient scribes address this by generating a structured draft during the visit. The workflow has three steps: record (software captures the session), edit (AI generates a note the clinician reviews and adjusts), and finish (clinician approves before the note enters any record).
A multicenter study of 263 ambulatory clinicians across six health systems found burnout dropped from 51.9% to 38.8% after 30 days of ambient scribe use, a 74% reduction in odds of burnout.⁴ A 63-week analysis across 7,260 physicians found high users saved 2.5 times more time per note than low users.5
A study of ten primary care physicians in the top 20% of EHR time outside scheduled hours found the most significant change was a reduction in characters typed, with same-day chart closure declining slightly.6 AI scribes may not benefit every clinician profile equally.
Clinical decision support
Clinical decision support (CDS) tools are software systems embedded in or alongside the EHR that analyze patient data in real time and surface relevant clinical information at the point of care. In primary care, this means flagging potential drug interactions when a prescription is written, identifying patients overdue for preventive screenings, surfacing differential diagnoses based on documented symptoms and labs, or alerting a clinician when documented findings are inconsistent with a current treatment plan. The tools do not make decisions. They present information the clinician uses to decide.
About 5% of US outpatient patients experience a diagnostic error annually, and 33% of those lead to permanent severe injury or death.7 A 2025 scoping review of 73 empirical studies found AI tools in primary care showed strong technical accuracy in diagnostic decision support, but implementation was limited by usability barriers, workflow misalignment, and clinician trust concerns.8
A separate scoping review found only six studies of AI-CDSS tested in real primary care clinical settings, covering diagnosis support, management recommendations, and complication prediction. Most algorithms remain in validation phases.⁹
Patient inbox and message management
Patient portal inbox volume has grown into a significant source of after-hours EHR work for primary care physicians. Patients send messages about symptoms, medication questions, referral requests, and test result interpretation. Each requires requiring the physician to review the record, formulate a response, and document the interaction. AI inbox tools draft a response based on the patient message and the recent chart. The physician reviews the draft before sending, rather than composing from scratch.
A Stanford quality improvement study of 162 clinicians found AI-drafted replies had a 20% utilization rate, with statistically significant reductions in burden and burnout scores, but no change in time spent.9
A simulation study found 80% of PCPs agreed AI drafts reduced cognitive workload, but 35–45% of drafts containing errors were submitted entirely unedited.10
Chronic disease management
Primary care panels carry a high volume of patients with ongoing conditions (diabetes, hypertension, COPD, heart failure) who need regular monitoring, medication adjustments, and preventive care follow-up. AI clinical tools in this category help practices track which patients are overdue for labs or screenings, predict which patients are at risk of deterioration, and flag gaps in care across the panel. Rather than relying on a clinician to remember or manually review the panel, these tools surface the information at the point of care or through a dashboard.
Chronic disease management represented 22% of AI primary care studies in the 2025 JMIR scoping review.8 Most evidence comes from large health system deployments. Population-level tools that monitor large patient panels need EHR infrastructure that surfaces analytics. Independent and group practices have limited data on this category.
Prior authorization
Prior authorization requires a practice to submit clinical documentation to a payer before certain medications, procedures, or referrals are approved. For primary care, this involves pulling the relevant records, matching the clinical justification to the payer’s coverage criteria, submitting the request, and tracking its status. This process can take 30 minutes to several hours per case depending on complexity and payer. AI tools in this category automate the population of authorization forms using existing chart data, match documentation to payer criteria, and track submission status.
For a practice without a dedicated authorization coordinator, this work typically falls on clinical staff or the physician. Small practices should evaluate authorization volume and payer mix before committing to a standalone tool versus relying on EHR-embedded workflows.
What do practices worry about when evaluating AI?
The AMA’s 2024 survey found 87% of physicians cited data privacy assurances and 84% cited EHR integration as top attributes needed to advance AI adoption.3 Peer discussions in r/FamilyMedicine and r/medicine surface additional operational concerns specific to smaller practices.11
- Setup without IT support. Tools need to work on existing hardware without a dedicated IT resource.
- EHR integration. Many practices use copy-paste rather than native write-back. The tool needs to produce output that gets into the chart without extra steps.
- HIPAA and data handling. BAA terms, storage location, retention period, and access rights.
- Accuracy in complex visits. Multi-problem primary care visits are where error risk is highest across all AI categories.
- Pricing transparency. Flat monthly fees are preferred over usage-based models that become unpredictable at higher patient volume.
Where should a practice start with AI?
Documentation has the strongest evidence and the lowest setup barrier. Start there.
After documentation, the next category depends on the practice’s specific constraint. High prior auth volume: evaluate authorization AI. Heavy patient portal message volume: trial inbox AI. Chronic disease panels with care gap compliance requirements: evaluate population health tools.
How does Commure Scribe support AI documentation in primary care?
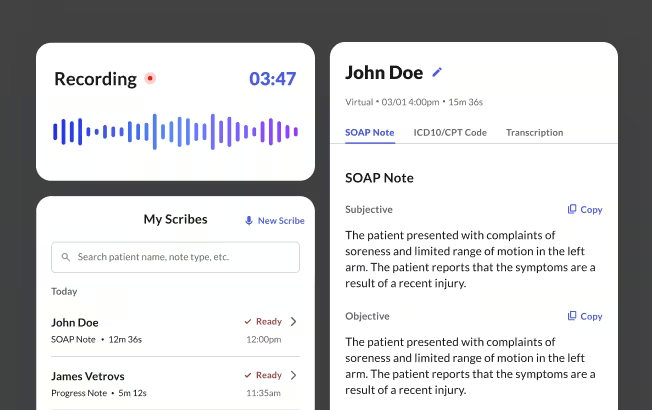
Commure Scribe is an ambient AI medical scribe for outpatient documentation. The clinician records the visit, the AI generates a structured SOAP note, and suggested ICD-10 and CPT codes appear in a separate tab. The codes are suggestions, not auto-entries. The clinician reviews and finalizes before anything posts to the record.
The Capture, Edit, Finalize workflow is consistent across visit types. A 7-day free trial covers a representative sample, including multi-problem encounters.
For independent and small practices, the standard workflow uses copy-paste into the EHR. Commure Scribe integrates with eClinicalWorks, Athenahealth, AdvancedMD, Elation, Practice Fusion, SimplePractice, Tebra, Cerbo, Kipu, and WebPT. Medium and large group practices access one-click EHR sync with custom workflows and live onboarding.
Additional details:
- 90 languages, automatic detection, no manual selection required
- In-person and telehealth encounters supported
- Family Medicine and Internal Medicine among supported specialties
- Audio stored, encrypted, HIPAA compliant. Not used for AI training. Default retention 1 year active, archived minimum 6 years.
- BAA available
How do you evaluate an AI tool for your practice?
Six steps, in order.
- Week 1: Run it on complex visits. Include multi-problem chronic care encounters, not just straightforward acute visits.
- Week 1: Verify the BAA and data terms. Confirm storage location, retention period, and access rights before the trial ends.
- Week 2: Test on your actual hardware. Use the device you use in exam rooms. Demo-environment performance is not representative.
- Week 2–3: Check EHR compatibility. Confirm copy-paste or native write-back availability and test with your most common note types.
- Week 3–4: Evaluate note quality directly. Compare AI drafts to your own notes on the same visit. Focus on the Assessment and Plan on multi-problem visits.
- Before committing: confirm pricing terms. Identify what triggers a price increase as volume grows.
Frequently Asked Questions
No. Documentation tools draft notes, clinicians review and finalize. Decision support surfaces options, clinicians decide. Inbox AI drafts messages, clinicians edit before sending.
Most documentation and inbox AI tools are designed for self-service setup. The clinician or office manager installs the tool and begins using it the same day.
Start with the highest-friction task in the current workflow. For most independent and group practices, that is documentation. Run a 7-day free trial on a mixed set of visit types, including multi-problem chronic care visits. Verify BAA terms and data handling before the trial ends.
Ambient documentation has the widest deployment, with 66% of physicians reporting AI use in 2024.³ Clinical decision support, patient inbox AI, and chronic disease management tools are in earlier stages of real-world primary care adoption. Prior authorization automation is being adopted by practices with high authorization volume.
AI inbox tools lower the effort of responding to patient messages, but they create a review problem. A simulation study found that 35–45% of drafts containing errors were submitted entirely unedited by PCPs. The errors included objective inaccuracies and harmful omissions. Every draft needs to be read before it is sent.
A multicenter study across six health systems found burnout dropped from 51.9% to 38.8% after 30 days of ambient scribe use.4 A 63-week large-scale analysis found high users saved 2.5 times more time per note than low users.⁵ A study of high-burden primary care physicians found the most significant change was a reduction in characters typed, with same-day chart closure declining slightly.6
Sources
1. Arndt BG, Beasley JW, Watkinson MD, et al. Tethered to the EHR: primary care physician workload assessment using EHR event log data and time-motion observations. Annals of Family Medicine. 2017;15(5):419-426. doi:10.1370/afm.2121. https://www.annfammed.org/content/15/5/419
2. Berg S. Burnout on the way down, but "pajama time" stands still. American Medical Association. August 13, 2024. https://www.ama-assn.org/practice-management/physician-health/burnout-way-down-pajama-time-stands-still
3. Berg S. 2 in 3 physicians are using health AI—up 78% from 2023. American Medical Association. February 2025. https://www.ama-assn.org/practice-management/digital-health/2-3-physicians-are-using-health-ai-78-2023
4. Olson KD, Meeker D, Barker TD, et al. Use of ambient AI scribes to reduce administrative burden and professional burnout. JAMA Network Open. 2025;8(10):e2534976. doi:10.1001/jamanetworkopen.2025.34976. https://pmc.ncbi.nlm.nih.gov/articles/PMC12492056/
5. Tierney AA, Gayre G, Hoberman B, et al. Ambient artificial intelligence scribes: learnings after 1 year and over 2.5 million uses. NEJM Catalyst. 2025. doi:10.1056/CAT.25.0040. https://permanente.org/analysis-ai-scribes-save-physicians-time-improve-patient-interactions-and-work-satisfaction/
6. Alpert JM, Saper R, Boose E, et al. Evaluating an artificial intelligence scribe for clinical documentation. Digital Health. 2025;11:20552076251395588. doi:10.1177/20552076251395588. https://pmc.ncbi.nlm.nih.gov/articles/PMC12638734/
7. Gomez-Cabello CA, Borna S, Pressman S, Haider SA, Haider CR, Forte AJ. Artificial-intelligence-based clinical decision support systems in primary care: a scoping review of current clinical implementations. European Journal of Investigation in Health, Psychology and Education. 2024;14(3):685-698. doi:10.3390/ejihpe14030045. https://pmc.ncbi.nlm.nih.gov/articles/PMC10969561/
8. Katonai G, Arvai N, Mesko B. AI and primary care: scoping review. Journal of Medical Internet Research. 2025;27:e65950. doi:10.2196/65950. https://pmc.ncbi.nlm.nih.gov/articles/PMC12368388/
9. Garcia P, Ma SP, Shah S, et al. Artificial intelligence-generated draft replies to patient inbox messages. JAMA Network Open. 2024;7(3):e243201. doi:10.1001/jamanetworkopen.2024.3201. https://pmc.ncbi.nlm.nih.gov/articles/PMC10955355/
10. Biro, J.M., Handley, J.L., Malcolm McCurry, J. et al. Opportunities and risks of artificial intelligence in patient portal messaging in primary care. npj Digit. Med. 8, 222 (2025). https://doi.org/10.1038/s41746-025-01586-2
11. r/FamilyMedicine. Time to close charts. Reddit. 2024. https://www.reddit.com/r/FamilyMedicine/comments/1ealzex/time_to_close_charts/, r/FamilyMedicine. Which AI tool is the best for primary care? Reddit. 2025. https://www.reddit.com/r/FamilyMedicine/comments/1pftct2/