





EHR Integration API: A Complete Guide
Standards, use cases, compliance requirements, and practical next steps for developers and practice leaders
Written by the Commure Scribe Team
Published: June 13, 2026
•
10 min read
Updated June 25, 2026
What You Need to Know About EHR Integration APIs
- EHR integration API connects external apps to electronic health records, enabling real-time data exchange through standard interfaces.
- Nine in 10 U.S. hospitals use APIs for patient data access, but many face obstacles moving from adoption to production use.¹
- Connecting an EHR to clinical tools, including AI scribes, can reduce documentation time and admin burden across the visit.
What is EHR integration API?
An EHR integration API is the programmatic interface a software application uses to read patient data from, and write it back to, an electronic health record system. It sits at the center of two converging pressures. The first is regulatory. In 2020, ONC required certified EHR vendors to offer standardized APIs for patient data access.³ The CMS Interoperability and Prior Authorization Final Rule added operational deadlines starting January 1, 2026.² Connected systems must now support automated workflows, including prior authorization.
The second is clinical. Care now spans more apps, devices, and care sites than any single EHR manages on its own. APIs are how labs, imaging platforms, billing tools, and clinical decision support software exchange data with the patient record.
These two pressures affect developers and practice leaders differently. Developers need to know which standards apply and where vendor versions differ. Practice leaders need a clear picture of setup requirements, compliance obligations, and the link between integration and clinical outcomes.
ONC data shows that most hospitals have adopted APIs for patient access, but many face real obstacles using them for efficient data exchange.¹ That gap between adoption and production use shapes every decision that follows. The key questions are which standard to build on, how to handle authentication, and what compliance actually needs.
How does EHR integration API work?
An EHR integration API follows a six-step cycle every time an external app requests data. Understanding each step helps both developers and practice leaders evaluate where integrations succeed or break down.
The steps are:
- Request. The external app sends a formatted API call to the EHR, specifying what data it needs and in which format.
- Authentication. The EHR checks whether the requesting app has valid credentials. Most EHR systems use SMART on FHIR, which runs OAuth 2.0 authorization to issue a time-limited access token.
- Retrieval. The EHR locates the requested patient data in its records.
- Transformation. The EHR formats the data as a FHIR resource, such as a Patient, Observation, or Medication object.
- Validation. The system checks that the response meets the agreed schema before sending.
- Response. The formatted data returns to the requesting app.
Authentication is where most production integrations struggle. SMART on FHIR tokens expire, and apps must handle refresh flows without interrupting the clinical workflow. Rate limits vary by vendor. EHR-specific quirks in how OAuth scopes are interpreted can mean a flow tested in sandbox behaves differently in production.
Testing environments often don't reflect production conditions. A 2024 survey of digital health companies found that 4 in 10 cited a lack of realistic clinical testing data as a substantial barrier to EHR API implementation.⁵
What standards govern EHR integration API?
Three standards govern most EHR integration API builds, and each serves a different purpose. For a deeper breakdown, see this overview of the HL7 and FHIR standards.
HL7 v2 has been the backbone of clinical data exchange for over 25 years. It handles lab results, admissions, discharges, and transfer messages across most live hospital systems. About 95% of U.S. healthcare organizations still use HL7 v2 for at least some workflows.⁴ If an integration touches legacy systems or high-volume lab messaging, HL7 v2 is likely in scope.
FHIR R4 is the current ONC-mandated standard for patient data access.³ It uses REST APIs, JSON, and XML, which makes it far easier to build on than older HL7 formats. FHIR breaks a patient record into modular resources: Patient, Observation, MedicationRequest, Encounter, and others. New integrations, especially those involving patient-facing apps or payer data exchange, should build on FHIR R4.
SMART on FHIR adds the authorization layer on top of FHIR. It extends OAuth 2.0 with healthcare-specific scopes. Apps can request access to specific data types, such as medications or lab results, without touching the full record. This framework is required for patient-facing app access under the ONC rules.³
The practical question is which standard the target EHR uses and how closely that matches the spec. Vendor deviations from the FHIR R4 spec are common and often undocumented.
What are the main benefits of EHR integration API?
EHR integration API delivers value across three areas: clinical workflow, patient experience, and compliance readiness.
On the clinical side, real-time data exchange means lab results, imaging reports, and medication changes reach the clinician without manual lookup or re-entry. API-connected tools, including clinical decision support, AI scribes, and remote monitoring platforms, can pull and push data without the clinician leaving the EHR workflow. Reduced manual entry also means fewer transcription errors in the patient record.
For patients, APIs power the apps that give them access to their own health data. Patients can view records, share data with specialists, and connect personal health apps to their care history. That access is now a federal right under ONC's information blocking rule.³
On the compliance side, EHR integration API is increasingly a requirement. The ONC information blocking rule needs certified EHR vendors to make patient data available through standardized APIs.³ The CMS Prior Authorization API mandates that payer-connected systems support automated prior auth workflows starting in 2026.² Practices without these connections will face operational gaps as deadlines take effect.
Each new EHR integration API connection adds to a shared data layer that makes next connections faster to build and more useful to the clinician.
What challenges should teams expect?
Teams should expect five recurring challenges: production-readiness gaps, trust framework setup, data normalization, limited in-house resourcing, and cost and timeline overruns. The first and most common is the gap between "FHIR-compliant" and "production-ready." A vendor can meet the ONC certification criteria while still using FHIR R4 in ways that need significant extra work. Missing resource types, non-standard extensions, and undocumented rate limits are common across major EHR vendors.
Trust framework gaps create a second category of problems. For two systems to exchange data via FHIR, they must establish a bilateral trust relationship. This typically happens through a vendor credentialing or app registration process.¹ That process can take weeks to months for large EHR platforms. It must be repeated for each organization. Without an established trust relationship, data access is blocked regardless of which standards are in place.
Data normalization is harder than data access. Even when two systems both use FHIR R4, they may represent the same clinical concept differently. A diagnosis coded one way in one EHR may need mapping before it is usable in another system. Teams that budget only for the API connection often underestimate the time spent on normalization.
Smaller practices face a resourcing gap that larger organizations do not. Building and maintaining an EHR integration needs in-house expertise in OAuth 2.0, FHIR resource models, and EHR-specific vendor behavior. Many independent and small group practices do not have that capability on staff, which is why middleware platforms and pre-built integration layers have grown.
Cost and timeline overruns are common. Multi-system EHR integration projects require budgeting beyond the API connection to cover data normalization, security review, testing, and ongoing maintenance. These additional phases regularly extend both timelines and total cost.
What are the most common use cases?
The most common use cases are patient data access apps, prior authorization automation, clinical decision support, AI-assisted documentation, population health analytics, and revenue cycle tools. These span clinical care, operations, and patient access.
Patient data access apps are the most widely deployed use case. ONC's information blocking rule needs EHRs to give patients access to their own data through standardized APIs.³ This powers consumer-facing apps. Patients can view records, share data with other providers, and connect personal health devices to their care history.
Prior authorization automation is the use case with the most immediate regulatory pressure. The CMS Interoperability and Prior Authorization Final Rule needs impacted payers to use a Prior Authorization API starting January 1, 2026.² That API allows providers to check whether prior auth is needed and retrieve documentation requirements. Requests go directly from the EHR, cutting the back-and-forth that delays care.
Clinical decision support tools use EHR APIs to pull real-time patient data. They surface alerts, drug interaction checks, and care gap notifications at the point of care.
AI-assisted documentation tools, including ambient AI scribes, use EHR APIs to read encounter context and write structured notes back to the record. For practices using these tools, a reliable EHR API connection determines whether documentation workflows run without manual copy-paste steps.
Population health and analytics platforms aggregate data across patients through batch API calls, powering dashboards for quality measures, chronic disease tracking, and value-based care reporting.
Revenue cycle tools use EHR APIs to pull encounter data for coding, billing, and claims submission, reducing manual charge entry and improving code accuracy.
What compliance requirements apply?
Three federal frameworks set the compliance floor for EHR integration API. Each applies to different participants in the data exchange chain.
The ONC Information Blocking Rule targets EHR vendors, health information networks, and healthcare providers. Covered actors may not block the exchange or use of electronic health information.³ The rule comes from the 21st Century Cures Act, with the compliance date taking effect April 2021 and civil monetary penalty enforcement beginning September 1, 2023. Penalties for health IT developers who violate the rule can reach $1 million per violation.
The CMS Interoperability and Prior Authorization Final Rule applies to impacted payers. It requires them to implement FHIR R4-based APIs for prior authorization, patient access, and payer-to-payer data exchange.² Operational and procedural requirements took effect January 1, 2026. All FHIR API implementation requirements are due January 1, 2027.² Providers and EHR vendors connecting to these payer systems must support the corresponding API workflows.
HIPAA's Security Rule applies to all covered entities and business associates involved in EHR integration APIs. Key requirements include:
- Encrypting data in transit and at rest (an addressable specification under the Security Rule, where covered entities must implement it or document an equivalent alternative)
- Maintaining audit logs for all API access
- Applying minimum necessary access when scoping OAuth permissions
- Executing Business Associate Agreements with third-party app developers who handle protected health information
State-level requirements add another layer. Some states impose stricter rules on patient consent or specific data types such as mental health or substance use records. Teams building integrations that touch these data categories should review state law in addition to federal frameworks.
How do you get started?
The starting point for EHR integration API depends on your role in the process.
For developers, the practical path starts with four questions:
- Which standard does the target EHR support? Most new builds should target FHIR R4. If the target system runs on HL7 v2 for core messaging, plan for both.
- What sandbox access is available? eClinicalWorks, Athenahealth, and most major EHR vendors offer developer programs with sandbox environments. Register early. Production review timelines vary and can extend several months.
- How will you handle authentication? Set up SMART on FHIR credentials, plan your token refresh strategy, and test scope handling before production. OAuth flows that work in sandbox often need adjustments for production-specific rate limits and session policies.
- What does production review need? Large EHR vendors typically need a security review, data use agreement, and sometimes a formal app certification before granting production access.
For practice leaders, the evaluation starts with a different set of questions:
- Which EHRs do you need to connect to, and do they expose FHIR R4 endpoints? Most certified EHR vendors are now required to.³ If you are still selecting a platform, weigh integration support alongside the other criteria covered in this guide to the best EMR software.
- Build or buy? Custom integrations give more control but need technical staff and long timelines. Middleware platforms and pre-built connectors reduce that burden for most outpatient workflows.
- What are your compliance obligations? If your payer contracts are affected by the CMS 2026 prior auth mandates, that timeline is not negotiable.²
- What is the realistic cost and scope? Get estimates that include the API connection, data normalization, testing, security review, and ongoing maintenance.
The best starting point for either role is a current list of the EHR integration APIs your target vendor exposes, including any known deviations from the FHIR R4 spec, and a clear understanding of which use case the integration needs to serve first.
How Commure Scribe connects to your EHR
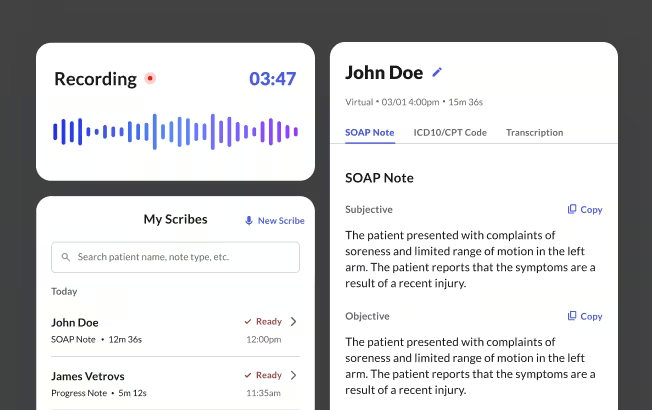
Commure Scribe is a practical example of the downstream benefit an EHR integration API delivers. It connects to 60+ EHR integrations, including eClinicalWorks, Athenahealth, and AdvancedMD, across independent practices, group practices, and health systems. The clinician records the encounter, and within seconds a structured clinical note appears, with suggested ICD-10 and CPT codes generated in a separate tab. The clinician reviews and approves before anything enters the chart, following a Capture, Edit, and Finalize workflow.
The integration layer is where the time savings come from. For larger groups, one-click EHR sync sends the finished note directly to the chart through the API connection, with no copy-paste step after the encounter. Smaller practices can sync via copy/paste with any EHR. Either way, the API handoff is what lets an AI medical scribe write structured notes to the record without manual re-entry, the exact workflow gain this guide describes.
90%+ of providers using Commure Scribe reduce their clinical documentation time and digital fatigue, a pattern that holds across 25M+ patient encounters annually. For practices evaluating EHR integration API, that downstream documentation workflow is often the use case the connection is built to serve first.
Frequently asked questions
What is the difference between FHIR and HL7?
HL7 v2 is the older messaging standard. It has transmitted lab results, admissions, and clinical events for over 25 years. Both are relevant to any EHR integration API build. FHIR R4 is the newer REST-based standard, now required by ONC for patient data access. Most organizations run both. HL7 v2 handles legacy workflows; FHIR R4 handles new integrations and patient-facing app access.
How long does EHR integration API take?
EHR integration API timeline varies by scope, EHR vendor, and whether the project needs app certification. Simple integrations against a well-documented FHIR R4 endpoint can move faster. Projects involving large EHR vendors, production review processes, or multiple system connections typically take several months to over a year.⁵
Is EHR integration API required by law?
For certified EHR vendors, some EHR integration API requirements apply by law. ONC needs them to provide standardized APIs for patient data access under the 21st Century Cures Act.³ For impacted payers, the CMS 2026 rule mandates specific FHIR-based APIs. For individual practices, direct requirements depend on payer contracts and the workflows in scope. Consulting a compliance advisor is recommended.
What is SMART on FHIR?
SMART on FHIR is an authorization framework built on top of FHIR and OAuth 2.0. It adds healthcare-specific permission scopes. Apps can request access to specific data types, such as medications or lab results, without accessing the full record. It is the standard auth layer for patient-facing apps and is required under ONC rules for that use case.³
How does EHR integration reduce documentation time?
When clinical tools connect via an EHR integration API, data flows automatically between systems. An AI scribe, for example, can write a structured note directly to the EHR without manual copy-paste. Billing tools can pull encounter data for coding without re-entry. Each automated handoff removes a manual step from the clinician's workflow, compressing the time between patient visit and closed chart.
This article is for general informational and educational purposes only. It does not constitute legal, medical, or professional advice and does not guarantee compliance. Requirements vary by state, payer, and clinical setting and can change over time. Verify current details with your own compliance officer, legal counsel, or the relevant authority before relying on this information.
Sources
- ONC Health IT. "Hospital Use of APIs to Enable Data Sharing Between EHRs and Apps." https://healthit.gov/data/data-briefs/hospital-use-apis-enable-data-sharing-between-ehrs-and-apps/ 2023
- CMS. "APIs and Relevant Standards and Setup Guides." https://www.cms.gov/priorities/burden-reduction/overview/interoperability/setup-guides-standards/application-programming-interfaces-apis-relevant-standards-setup-guides-igs 2024
- ONC Health IT. "Understanding Emerging API-Based Standards." https://isp.healthit.gov/understanding-emerging-api-based-standards 2023
- National Library of Medicine. "Health Data Standards and Terminologies: Version 2 (V2)." https://www.nlm.nih.gov/oet/ed/healthdatastandards/03-300.html 2024 (citing HL7 Version 2 Product Brief)
- ONC Health IT. "Digital Health Company Experiences Using EHR APIs." https://healthit.gov/blog/research-and-scientific-advancement/digital-health-company-experiences-using-ehr-apis/ 2024





