





Mental Health Questionnaire: 3 Free Templates
A PHQ-9 depression form, a GAD-7 anxiety form, and a blank shell for other validated instruments, with the structure, scoring, and documentation standards behind each.
Written by the Commure Scribe Team
Published: May 28, 2026
•
8 min read
Updated June 11, 2026
What You Need to Know About Mental Health Questionnaires
- Mental health questionnaires are validated screeners, not diagnostic tests, and scores guide next steps in care.²,⁷
- An instrument is only valid for the population it was tested in; extrapolation should be documented.⁸
- Three printable forms ship with this guide: a PHQ-9 depression questionnaire, a GAD-7 anxiety questionnaire, and a blank shell for other validated instruments.⁵,¹¹
What is a mental health questionnaire?
A mental health questionnaire is a structured, validated instrument. It captures how a patient reports symptoms, feelings, or daily functioning across defined mental health domains. Practices use these questionnaires as screening or monitoring tools rather than diagnostic tests. Items come from a validated scale and are scored against published thresholds. Scores are interpreted alongside clinical history and examination.⁴,⁷
Mental health questionnaires cover two overlapping tool types. Patient-completed scales such as the PHQ-9 or GAD-7 sit inside routine primary care and specialty visits. Longer multi-domain instruments such as the Positive Mental Health Questionnaire support surveillance or workplace programs.⁷
Most validated mental health questionnaires share four components:
- Instructions
- Likert-style items
- A scoring key
- A decision rule that specifies follow-up
The sections below cover instrument selection, structure and scoring, validation, where questionnaires fit in care, documentation and compliance, and a usable template.
Which mental health questionnaires are most widely used, and what does each measure?
Practices choose from a small set of validated mental health questionnaires, each scoped to a specific condition, population, or dimension of functioning. Short depression and anxiety scales anchor primary care screening. Longer instruments support periodic wellness monitoring or workforce-specific use.
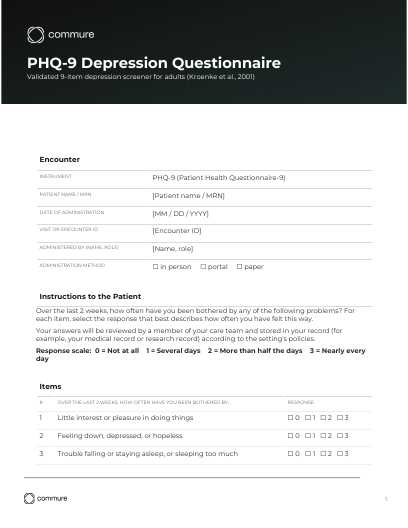
The PHQ-9 (Patient Health Questionnaire-9) is a widely used depression screener in primary care.⁵ It is validated for use in adults; a modified version, the PHQ-A, is used for adolescents. The PHQ-9 has 9 items aligned with the diagnostic criteria for major depressive disorder, a fixed "over the last 2 weeks" recall window, and a 0–3 response scale per item. Total scores run from 0 to 27 and map to five severity bands:⁵
- 0–4: minimal depression
- 5–9: mild
- 10–14: moderate
- 15–19: moderately severe
- 20–27: severe
Question 9 asks about thoughts of self-harm and should trigger a focused risk assessment when endorsed.⁵
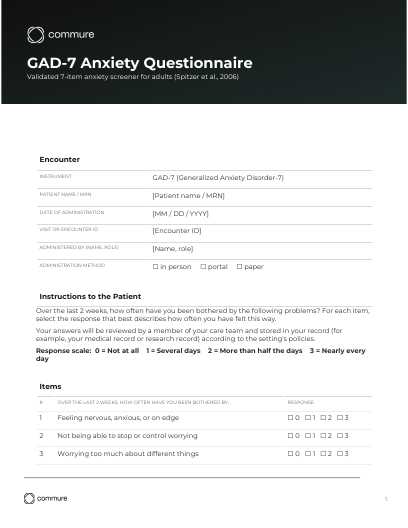
The GAD-7 (Generalized Anxiety Disorder-7) is the companion anxiety screener.¹¹ It is validated for use in adults. The GAD-7 has 7 items, the same "over the last 2 weeks" recall window and 0–3 response scale as the PHQ-9, and total scores from 0 to 21 mapped to four severity bands:¹¹
- 0–4: minimal anxiety
- 5–9: mild
- 10–14: moderate
- 15–21: severe
The Positive Mental Health Questionnaire takes a different approach. Instead of screening for symptoms, it measures indicators of mental well-being across several domains.⁷,⁸ Domains include:
- Life satisfaction
- Interpersonal relationships
- Self-control
- Autonomy
- Problem-solving
It has been validated with healthcare workers and university student populations and supports periodic monitoring rather than acute diagnosis.
The Nurse's Workplace Mental Health Questionnaire measures workplace-related mental health strain in nurses across three dimensions:⁶
- Occupational
- Interpersonal
- Organizational
Population-level mental health surveillance programs combine multiple validated screeners to track risk and outcomes over time.⁹
How are mental health questionnaires structured and scored?
A mental health questionnaire gives reproducible results because its components follow a predictable structure. The instrument specifies how items are worded, how the patient responds, and how responses convert into a score. Practices that deviate from the original structure risk producing scores that are not comparable to the validation data.⁸
Responses are typically recorded on a Likert-style scale.⁶,⁸ Scales range from strongly disagree to strongly agree or from never to always. Item scores sum into subscale totals and an overall score that clinicians compare to published thresholds. Interpretation follows the decision rule published with the instrument. That rule specifies what scores indicate low, moderate, or high levels of the construct being measured.
Government forms embed the same structure but expose it more visibly. The Iowa Adult Mental Health Questionnaire, Form 470-5773, opens with identifying information and instructions. It then presents numbered items with response fields and closes with an area for scoring or narrative response.⁴ The Oklahoma Department of Corrections Group Administered Mental Health Questionnaire uses the same pattern for a correctional population.¹⁰
What makes a mental health questionnaire valid for clinical use?
A mental health questionnaire is valid when published studies confirm the instrument measures what it claims. The validation must be specific to the population where the instrument will be used. Reliability and validity are the two psychometric properties clinicians should look for before adopting an instrument.
Reliability is the degree to which scores are stable and consistent. Internal consistency is measured when the items on a scale move together in expected ways.⁶,⁷ Test-retest reliability is measured when scores remain stable across administrations, absent a real change in the underlying construct.
Validity is the degree to which scores reflect the construct in question. Factor analysis confirms whether items group into the expected domains.⁶,⁸
Population and setting matter: an instrument validated in nurses may not perform the same way in general adult primary care.⁶ Clinicians should match the mental health questionnaire to the population described in the validation study. Any extrapolation to a different population should be documented.⁷
Where do mental health questionnaires fit in a care pathway?
Mental health questionnaires attach to three distinct points in a care pathway, each with its own administration, review, and response workflow.
Intake screening catches undiagnosed or emerging mental health concerns before the clinician enters the room. Patient-completed forms administered in the waiting area or patient portal generate scores that shape the agenda for the visit.⁴ A positive screen directs the clinician to a more focused mental health assessment or warm handoff to behavioral health.
In-visit monitoring tracks response to treatment in patients with known diagnoses. Repeated administrations of the same mental health screening questionnaire produce score trends that support medication adjustment and psychotherapy planning.² Harvard Health Publishing describes this longitudinal use as central to the purpose of contemporary mental health questionnaires.³
Surveillance extends the instrument to a population rather than an individual visit. Programs that serve correctional facilities or public health populations use validated scales at scale. The aggregated scores detect clusters of need, guide resource allocation, and evaluate program outcomes.⁹,¹⁰ Workplace mental health screening of employees is more constrained: medical inquiries to employees are restricted under the Americans with Disabilities Act, and any program should be voluntary, confidential, and structured to comply with ADA and state employment law.
What documentation and compliance requirements apply to a mental health screening questionnaire?
Administering a mental health questionnaire creates three obligations practices should meet consistently:
- Documentation
- Consent
- Response protocol
These obligations span clinical, quality, and regulatory requirements.
Documentation should capture the following:⁴,¹⁰
- The instrument used
- The date and administration method
- The full item-level responses
- The total and subscale scores
- The clinician's interpretation
A narrative note that ties scores to the clinical picture and next steps closes the record. Consistent documentation enables chart audits, quality reporting, and continuity of care across clinicians.
Consent and purpose must be clear to the patient. The patient should understand why the mental health questionnaire is being administered.³ They should also know what will be done with the results and what a positive screen triggers.
Response protocols for positive screens are part of ethical use. A mental health screening questionnaire is only as safe as the pathway that follows a positive result. Published programs specify escalation steps:⁶,⁹
- Focused clinical assessment
- Warm handoff to behavioral health
- Crisis intervention
- Referral
Regulatory and quality-program requirements can attach external obligations. The US Preventive Services Task Force gives a Grade B recommendation for depression screening in adults, including pregnant and postpartum patients,¹² and for anxiety screening in adults ages 19 to 64.¹³ Quality programs operationalize these recommendations. The HEDIS DSF-E measure (Depression Screening and Follow-Up for Adolescents and Adults) and the CMS MIPS quality measure Q134 both require documented screening with a follow-up plan when results are positive. Some state policies also mandate inclusion of mental health questionnaires inside health assessments.¹ Building these requirements into a clinical documentation improvement program closes the gap between audit expectations and day-to-day charting.
How does practice size change who owns each step?
The seven core steps of a mental health questionnaire program apply to every practice, but ownership and execution differ by size. Solo and small practices typically consolidate roles; medium and large groups distribute them across functions.
StepSolo and small practiceMedium group practiceLarge group practiceInstrument selectionClinician picks one screener (often PHQ-9 or GAD-7)Clinical committee selects screeners by care lineStandardized across all sites by clinical leadershipAdministrationPaper form at intake or in the exam roomPatient portal or tablet at intakePatient portal integrated with the EHR; tablet backupScoringManual scoring by clinician or MAAuto-scored inside the EHR templateAuto-scored, with real-time clinical decision supportDocumentationFree-text note plus score in the chartEHR template captures structured fieldsEHR template plus structured FHIR data for quality reportingResponse and follow-upClinician schedules follow-up per protocolCare coordinator manages follow-up across patientsPopulation health team monitors cohort follow-up ratesConsent and storageStandard treatment consent; chart-only storageDocumented consent process; EHR storage with audit logConsent management platform; EHR plus quality registryAudit and quality reportingFolder of administered forms reviewed annuallyCompliance lead audits a sample quarterlyCompliance and QI teams run continuous audits and report to payers
What does a mental health questionnaire template look like in practice?
A mental health questionnaire template gives a practice a reusable form the instrument's author would recognize. The template adds the administrative and compliance fields a chart audit expects. The anatomy breaks into seven sections:
- Header
- Instructions
- Items
- Scoring
- Interpretation
- Response
- Consent
The header identifies the encounter. It should include:⁴
- Patient name or identifier
- Date of administration
- Visit or encounter ID
- Administering staff role
- The exact name and version of the instrument
Version capture matters because scoring rules change across revisions of validated instruments.⁸
Instructions translate the instrument's prompt into language the patient can follow. This section should cover:³
- Reading level
- Response format explanation
- Recall window
- A statement about how the responses will be used
Item fields should follow three rules:⁶,⁸
- Items are numbered
- Wording matches the validation source
- Response options match the original Likert-style scale
Altered wording can compromise the instrument's psychometric validity.
The scoring section converts responses into numeric output. Subscale totals, the overall score, and any flagged critical items feed the clinician's interpretation line.⁷ A reusable template should include the scoring key so scoring does not depend on outside reference.
Interpretation and response sections turn the score into action. The clinician documents the interpretive category, such as minimal, mild, moderate, or severe. The note also captures the corresponding protocol step and the follow-up plan.⁹,¹⁰ For positive screens, the response row should name the next clinical action and the responsible party.
The consent row records three items:¹
- The purpose explanation
- The patient's consent
- The storage location for the completed mental health questionnaire
Three companion forms for download
This guide ships with three ready-to-use forms for download. Each form uses the same audit-ready structure (header, instructions, items, scoring, interpretation, response, and consent) and can drop into an EHR template builder or an intake packet:
- PHQ-9 depression questionnaire: 9 validated items, "over the last 2 weeks" recall window, 0–3 response scale, scoring bands 0–27.⁵
- GAD-7 anxiety questionnaire: 7 validated items, "over the last 2 weeks" recall window, 0–3 response scale, scoring bands 0–21.¹¹
- Blank instrument template: the seven-section shell with no items prefilled, for practices using other validated instruments (PMHQ, NWMHQ, or another).
Licensing note. The PHQ-9 and GAD-7 were developed with an educational grant from Pfizer Inc., which has made both instruments available without license fee for non-commercial clinical use with attribution to the developers.⁵,¹¹ Confirm current distribution terms on the instrument owner's licensing page (for example, ePROVIDE) before deployment.
How an AI medical scribe supports mental health questionnaire documentation
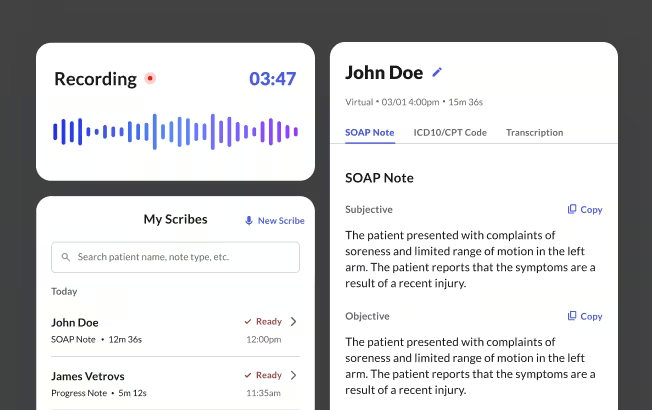
Commure Scribe is an ambient AI medical scribe that is HIPAA compliant and SOC 2 certified, with onshore data storage and 99.4% transcription accuracy. For practices running a mental health questionnaire program, Commure Scribe captures the clinical conversation around the instrument and turns it into structured, audit-ready documentation.
Immediately after the clinician clicks End Recording, a structured SOAP note appears within seconds. The note captures the full clinical context of the encounter, and suggested ICD-10 and CPT codes are generated alongside it. The clinician reviews, edits, and finalizes before anything posts.
Documentation compliance shows up in three ways for a practice that administers a mental health questionnaire:
- Commure Scribe captures the instrument name (for example, PHQ-9 or GAD-7), scores reviewed with the patient, and the clinician's interpretation inside the encounter narrative, so a chart audit can reconstruct the full decision pathway.
- Suggested ICD-10 and CPT codes surface in a separate tab for clinician review, so the final note can reflect the questionnaire-informed diagnosis and screening activity.
- Audio is encrypted in transit and at rest, retained per HIPAA requirements, and not used for model training, protecting the privacy of sensitive mental health content.
Commure Scribe does not replace the mental health questionnaire. It supports the practice by capturing the clinical context around its use so the documentation meets the standard a compliance or quality reviewer expects. For a ranked breakdown of AI scribe options by practice size and specialty, see the best AI medical scribes guide.
Mental Health Questionnaire Template Download
Download a copy of this template
Thanks! Your mental health questionnaire is ready.
Click below to download.
Thanks! Your PHQ-9 depression questionnaire is ready.
Click below to download.
Thanks! Your GAD-7 anxiety questionnaire is ready.
Click below to download.

Sources
- Connecticut General Assembly. (2015). An Act Concerning the Inclusion of a Mental Health Questionnaire in Health Assessments (HB 5988). https://www.cga.ct.gov/2015/TOB/H/2015HB-05988-R00-HB.htm
- Dowrick, C., Leydon, G. M., McBride, A., Howe, A., Burgess, H., Clarke, P., Maisey, S., & Kendrick, T. (2009). Improving care in depression: Qualitative study investigating the effects of using a mental health questionnaire. Quality in Primary Care, 17(4), 251–259. https://pubmed.ncbi.nlm.nih.gov/19807958/
- Harvard Health Publishing. (2016). What's the purpose of the new mental health questionnaire? Harvard Health Letter. https://www.health.harvard.edu/mental-health/ask-the-doctors-whats-the-purpose-of-the-new-mental-health-questionnaire
- Iowa Department of Health and Human Services. (n.d.). Mental Health Questionnaire (Form 470-5773). https://hhs.iowa.gov/media/6315/
- Kroenke, K., Spitzer, R. L., & Williams, J. B. W. (2001). The PHQ-9: Validity of a brief depression severity measure. Journal of General Internal Medicine, 16(9), 606–613. https://pubmed.ncbi.nlm.nih.gov/11556941/
- Lai, J., Zhang, R., Hong, M., & Li, N. (2022). Development and validation of the Nurse's Workplace Mental Health Questionnaire. International Journal of Nursing Sciences, 9(4), 521–528. doi:10.1016/j.ijnss.2022.09.004. https://pubmed.ncbi.nlm.nih.gov/36285083/
- Lapa, T. A., Madeira, F. M., Viana, J. F., & Pimentel, F. L. (2023). Positive Mental Health Questionnaire (PMHQ) for healthcare workers. Psychology Research and Behavior Management. https://pmc.ncbi.nlm.nih.gov/articles/PMC10706672/
- Lluch-Canut, T., Puig-Llobet, M., Sánchez-Ortega, A., Roldán-Merino, J., & Ferré-Grau, C. (2017). Reliability and validity of the Positive Mental Health Questionnaire in university students. Journal of Psychiatric and Mental Health Nursing. https://pubmed.ncbi.nlm.nih.gov/28150373/
- Meidl, V., Dallmann, P., Steffen, K., Bretthauer, B., Busch, A., Kubosch, E. J., Leonhart, R., & Hirschmueller, A. (2024). Mental health surveillance in elite Para athletes: Early identification and follow-up of athletes at risk of mental health problems. British Journal of Sports Medicine, 58(16), 902–909. doi:10.1136/bjsports-2023-107995. https://pmc.ncbi.nlm.nih.gov/articles/PMC11347970/
- Oklahoma Department of Corrections. (n.d.). Group Administered Mental Health Questionnaire (MSRM 140201.01.1). https://oklahoma.gov/content/dam/ok/en/doc/documents/policy/section-14/msrm/msrm_140201.01.1.pdf
- Spitzer, R. L., Kroenke, K., Williams, J. B. W., & Löwe, B. (2006). A brief measure for assessing generalized anxiety disorder: The GAD-7. Archives of Internal Medicine, 166(10), 1092–1097. https://pubmed.ncbi.nlm.nih.gov/16717171/
- US Preventive Services Task Force. (2023). Screening for Depression and Suicide Risk in Adults: US Preventive Services Task Force Recommendation Statement. JAMA, 329(23), 2057–2067. https://pubmed.ncbi.nlm.nih.gov/37338872/
- US Preventive Services Task Force. (2023). Screening for Anxiety Disorders in Adults: US Preventive Services Task Force Recommendation Statement. JAMA, 329(24), 2163–2170. https://pubmed.ncbi.nlm.nih.gov/37338873/





