





Superbill Template: What to Include, How to Use It, and When AI Can Do the Heavy Lifting
Required fields, compliance rules, specialty code lists, and a free downloadable template, plus how AI documentation reduces the manual coding step after every visit

Medically Reviewed by Donald Lazure
Written by the Commure Scribe Team
Published: May 9, 2026
•
14 min read
Updated June 11, 2026
What You Need to Know About Superbill Templates
- A superbill template is a receipt you give patients after a visit so they can seek direct reimbursement from their insurer. The practice does not file it. The patient does.
- Payers typically require: patient demographics, provider NPI and tax ID, ICD-10 diagnosis codes, CPT/HCPCS procedure codes, dates of service, fees, and a provider signature.
- Required fields are universal across specialties. What varies is the mix of CPT and ICD-10 codes, which is why pre-loading your most common codes into the template matters.
- For independent and group practices, the highest-friction step is code selection. AI medical scribes can surface suggested ICD-10 and CPT codes from the visit note, reducing that step to a review rather than a lookup.
What is a superbill, and when does a practice actually need one?
A superbill template is a structured document a provider gives to a patient after a visit. The patient submits it to their insurance company for direct reimbursement. It is not a claim. The practice does not file it on the patient's behalf.
A superbill is the right tool when a practice is out-of-network with a patient's insurer, when a patient has a PPO or POS plan with out-of-network benefits, or when a practice operates on a cash-pay model. Some patients also request superbill templates for FSA or HSA documentation, even when the practice does bill insurance.A superbill handles post-visit documentation. It does not replace the pre-visit obligation. Under the No Surprises Act (effective January 2022), providers are required to give uninsured and self-pay patients a Good Faith Estimate (GFE) before the visit occurs. The GFE must include expected charges for the visit. If the final bill exceeds the GFE by more than $400, the patient has grounds for a dispute. Cash-pay practices issuing superbills need both documents in their workflow: GFE before the visit, superbill after.
For independent and group practices, the superbill is often the entire billing interface with certain patient populations. A solo family medicine physician who does not accept insurance still has a professional obligation to give patients the documentation they need. Navigating out-of-network benefits without a complete superbill template is not straightforward for most patients.
What does a complete superbill template include?
The fields below represent the minimum required content for a superbill to be usable by a patient's insurer. Missing any of these often results in the claim being delayed, rejected, or returned for correction.
Patient information
- Full legal name
- Date of birth
- Address
- Insurance member ID and group number
- Name of insured (if different from patient)
Provider information
- Full legal name of rendering provider
- Practice name
- Practice address and phone number
- National Provider Identifier (NPI)
- Tax Identification Number (EIN or SSN)
- Provider Taxonomy Code (10-digit specialty code required by many payers, especially for specialty and behavioral health)
Visit and billing details
- Date(s) of service
- Place of service code (e.g., 11 for office, 02 for telehealth)
- ICD-10 diagnosis codes with sufficient specificity
- CPT or HCPCS procedure codes for each service rendered
- Modifiers, if applicable (e.g., 25 for a significant, separately identifiable E/M on the same day as a procedure)
- Fee charged for each service
- Amount paid by the patient (copay, self-pay payment)
- Balance due
- Referring provider name and NPI (required for specialist visits, PT, cardiology, imaging. Without this, the insurer will reject the claim)
- Assignment of benefits: state "Benefits are not assigned; please remit payment directly to the patient;" prevents the insurer from sending the reimbursement check to the practice instead of the patient
Signature and attestation
- Provider signature or printed name and credentials
- Date of signature
A note on ICD-10 specificity. Insurers routinely reject superbills that use non-specific or placeholder diagnosis codes. A code like Z00.00 may be accurate, but a superbill for a visit where hypertension was managed should also include I10. A non-specific code gives the insurer grounds to return the superbill. The patient must then contact the practice for a corrected version.
How do you create and deliver a superbill to a patient?
Completing a superbill template follows five steps for most independent practices. How long it takes depends on whether you are pulling codes manually or whether your documentation tools support suggested coding.
- Collect patient and insurance information at intake. The front desk or intake form should capture the insurance member ID, group number, and insured's name before the visit. Chasing this information post-visit adds friction and delays superbill delivery.
- Complete the clinical documentation first. The visit note must be done before you can select accurate codes. For manual code selection, review the note and match each diagnosis and procedure to the correct ICD-10 and CPT codes. If your documentation tool suggests codes from the encounter, review and confirm them.
- Populate the superbill template. Enter the visit and billing details. For practices using a static Word or PDF template, this is a manual step. For practices using an EHR with superbill functionality, some fields may auto-populate.
- Verify before delivery. Confirm that the NPI and tax ID are correct, that all services rendered have corresponding CPT codes, and that the fee column is complete. A completed superbill template returned for correction delays the patient's reimbursement and pulls admin time back into a closed visit.
- Deliver to the patient and retain a copy. Deliver the superbill template at checkout or securely by email. Keep a copy in the patient record.
Batching vs. per-visit superbills. For a solo clinician managing their own admin, batching superbill template completion to end-of-day or end-of-week reduces context switching. The tradeoff is that patients may have to wait. Most practices default to same-day delivery when volume allows.
Does a superbill template look different by specialty?
The required fields are universal. What changes by specialty is the mix of CPT codes and the ICD-10 codes pre-loaded in the superbill template.
Family medicine and internal medicine. Superbills are dominated by E/M codes (99202–99215), with chronic disease management codes (99490, 99491) and preventive visit codes (99385–99397) appearing frequently. Annual wellness visits (G0438, G0439) are Medicare-specific. ICD-10 codes for hypertension (I10), type 2 diabetes (E11.x), and hyperlipidemia (E78.x) appear in the majority of templates.
Psychiatry and behavioral health. E/M codes still apply for psychiatrists. Psychotherapy add-on codes (90833, 90836, 90838) and standalone psychotherapy codes (90832, 90834, 90837) are the center of most superbills. Telehealth modifier 95 is common. ICD-10 codes for major depressive disorder (F32.x, F33.x), anxiety disorders (F41.x), and ADHD (F90.x) are the most common diagnosis entries.
Physical therapy. PT superbills lean heavily on timed procedure codes (97110, 97530, 97150), evaluation codes (97161–97163), and re-evaluation codes (97164). The units column matters more here than in most specialties. Many payers now also require total session time in minutes, and sometimes start and stop times, on the superbill itself. Without total time documented, insurers may downcode the submitted units.
Speech-language pathology and audiology. SLP superbills often include evaluation codes (92521–92524) and treatment codes (92507, 92508). Audiology adds codes for audiometric testing (92551–92557).
For any specialty, the most common codes for your practice are worth pre-loading into your template. Doing so means the provider checks boxes or enters units rather than typing codes from memory at each visit.
What compliance rules apply to superbills?
Superbill errors carry the same compliance exposure as claim errors. The document carries patient PHI and drives a reimbursement decision. Inaccurate coding or missing provider identifiers is not just an administrative problem.
- Accuracy is mandatory. A superbill with a diagnosis code not documented in the visit note is not just an error. A procedure code for a service not rendered carries the same exposure. It can constitute misrepresentation to an insurer. Code what was documented, document what was done.
- Current codes only. CPT codes are updated annually by the AMA. ICD-10-CM codes are updated each October by CMS. Using a retired code can result in patient claim rejection.
- NPI and tax ID accuracy. Some practices have both an individual NPI (Type 1) and a group NPI (Type 2). Confirm which the patient's insurer requires before completing the superbill template.
- Superbills do not guarantee reimbursement. Out-of-network benefits, deductibles, and plan-specific exclusions all affect whether the patient receives reimbursement. This disclaimer belongs on any patient-facing template.Medicare opt-out status. Providers who have not formally opted out of Medicare cannot legally provide a superbill to a Medicare beneficiary for covered services. If you have opted out, note it on the superbill: "Provider has opted out of Medicare; no Medicare reimbursement is available for this visit." Failing to manage this correctly exposes both the provider and the patient to compliance risk.
How does AI documentation change superbill workflows for small practices?
The bottleneck is code selection. That means matching each service to the right CPT code. It also means identifying every ICD-10 code the visit supports.
For a solo clinician who sees 18 to 25 patients a day, selecting codes manually adds meaningful time to a compressed schedule. A 2023 JAMA Network Open study found that physicians spend nearly two hours on EHR and administrative tasks for every hour of patient care.⁴
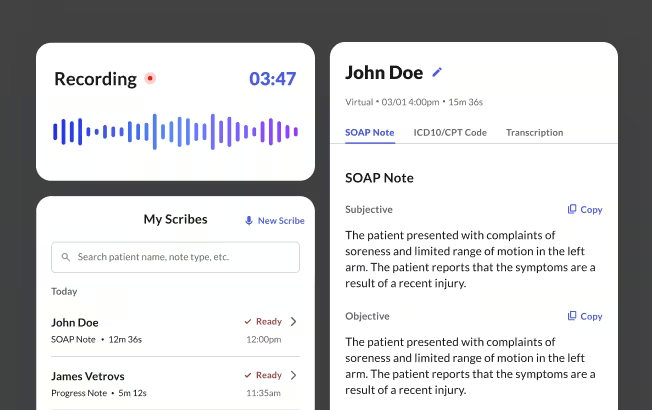
AI scribe tools and superbill accuracy. An ambient AI medical scribe captures the conversation during the encounter and generates a structured clinical note. AI scribe tools can surface suggested ICD-10 and CPT codes from that note, available immediately after the visit ends. The clinician reviews and confirms those suggested codes before they appear in any billing document.
AI scribes and EHR integration. When an AI scribe and an EHR integrate, the documentation workflow and the billing workflow collapse into one step. The scribe captures the encounter, generates the note, and surfaces suggested codes. The clinician reviews, then pushes the note directly into the EHR. The superbill template fields that depend on the visit note (diagnoses, procedures, dates of service) pull from the same source, with no re-entry.
How does Commure Scribe support superbill accuracy for independent and group practices?
For independent and group practices creating superbill templates without dedicated billing staff, coding accuracy depends on documentation completeness. A note that does not capture every diagnosis addressed produces an incomplete superbill template. Once the patient has left, corrections require additional contact.
Commure Scribe generates a structured SOAP note and surfaces suggested ICD-10 and CPT codes in a separate tab. The codes are available immediately after the visit ends. The clinician reviews and confirms before finalizing. The workflow is Capture, Edit, Finalize. Admin Copilot can also draft the superbill template directly from the encounter, pre-populating fields from the documented visit. The clinician reviews before anything is sent to the patient. A secondary benefit is medical necessity documentation. A common reason superbills are rejected by insurers is not a wrong code but an insufficient justification for that code in the underlying note. AI-generated notes tend to capture clinical reasoning more completely than manual notes under time pressure, which strengthens the patient's position if the insurer audits the visit later.
Coding accuracy starts with transcription accuracy. Commure Scribe operates at 99.4% transcription accuracy and supports 90 languages with automatic detection. It integrates with 60+ EHRs and EMRs, including one-click sync with AdvancedMD, eClinicalWorks, Athenahealth, Cerbo, Elation, SimplePractice, Tebra, Practice Fusion, WebPT, and Kipu. Copy/paste into any web-based EHR is also available. Fully HIPAA compliant and SOC 2 certified.
Free superbill template: general outpatient (all specialties)
The superbill template below covers the required fields for a general outpatient visit. For specialty-specific versions, use it as the base. Add the common CPT and ICD-10 codes for your specialty in the diagnosis and procedure rows.
SECTION
FIELD
PATIENT INFORMATION
Patient name / Date of birth / Address / Insurance member ID / Group number / Insured name (if different)
PROVIDER INFORMATION
Provider name / Practice name / Practice address / Practice phone / NPI (Type 1 and/or Type 2) / Tax ID (EIN or SSN)
VISIT DETAILS
Date of service / Place of service code / Referring provider NPI (if applicable)
DIAGNOSIS CODES
ICD-10-CM code 1 / DescriptionICD-10-CM code 2 / DescriptionICD-10-CM code 3 / Description
PROCEDURES / SERVICES
CPT/HCPCS code / Description / Modifier / Units / Fee
PAYMENT
Total charges / Amount paid by patient / Balance due
SIGNATURE
Provider signature / Printed name and credentials / Date
DISCLAIMER
Submission of this superbill to your insurer does not guarantee reimbursement. Coverage is subject to your individual plan terms, deductibles, and out-of-network benefits.
Superbill quality checklist for independent practices
Before giving a completed superbill template to a patient, confirm each of the following.
- Patient name and date of birth match insurance card
- Insurance member ID and group number are current (not from a prior plan year)
- NPI is correct for the rendering provider and, if applicable, the group
- Tax ID is the EIN or SSN associated with the billing entity
- All ICD-10 codes are from the current code set (updated October each year)
- Each ICD-10 code is specific to the encounter, no placeholder or unspecified codes where specificity is available
- Each CPT code corresponds to a service documented in the visit note
- E/M level selection is supported by the documented medical decision making or total time
- Modifiers are included where applicable (e.g., modifier 25, modifier 59)
- Fee column is complete for every CPT line
- Patient payment is recorded accurately
- Provider signature and date are present
- Disclaimer about reimbursement is included
- A copy has been retained in the patient record
Superbill Template Download
Download a copy of this template
Thanks! Your template is ready.
Click below to download

Frequently Asked Questions
No. An invoice is a request for payment from the practice to the patient. A superbill template is a detailed clinical and billing document the patient uses to request reimbursement from their insurer. An invoice lists what the patient owes you. A superbill template gives the insurer everything it needs to assess a claim.
Any licensed provider can issue a superbill, but the information on it must be accurate and match the services rendered. A provider does not need to be credentialed with a specific insurer to issue a superbill. The patient's coverage for out-of-network services determines whether reimbursement follows.
The patient submits the superbill template directly to their insurer, typically by mail or through the insurer’s online member portal. The insurer processes it as an out-of-network claim. Timely filing limits vary by insurer; most need submission within 90 to 365 days of the date of service.
The codes on a superbill template must reflect the actual diagnoses documented during the encounter and the services rendered. ICD-10 codes should be as specific as the documentation supports. CPT codes should match each distinct service provided. Using codes not supported by the visit documentation is a compliance violation regardless of the billing mechanism.
Yes. Telehealth superbills need the same fields as in-person superbills, with two additions. The place of service code should reflect telehealth: 02 or 10, depending on where the patient receives the service. Modifier 95 is commonly needed to indicate synchronous telehealth.
An AI scribe changes how the clinical note is generated, not the legal and professional obligations attached to the superbill. The provider still reviews and confirms any suggested codes before they appear on a billing document. What AI documentation can improve is the completeness of the underlying note, which directly supports more accurate code selection.
Sources
1. American Medical Association. CPT Code Set. https://www.ama-assn.org/practice-management/cpt.
2. Centers for Medicare and Medicaid Services. ICD-10-CM Official Guidelines for Coding and Reporting. https://www.cms.gov/medicare/coding-billing/icd-10-codes.
3. Centers for Medicare and Medicaid Services. Place of Service Codes. https://www.cms.gov/medicare/coding-billing/place-of-service-codes.
4. Arndt BG, Beasley JW, Watkinson MD, Temte JL, Tuan WJ, Sinsky CA, Gilchrist VJ. Tethered to the EHR: Primary Care Physician Workload Assessment Using EHR Event Log Data and Time-Motion Observations. Ann Fam Med. 2017 Sep;15(5):419-426. doi: 10.1370/afm.2121. PMID: 28893811; PMCID: PMC5593724. https://pubmed.ncbi.nlm.nih.gov/28893811/





