Insights for clinical leaders, physicians, nurses, and care teams focused on improving care delivery, reducing administrative burden, and enhancing the clinical experience.
5 Practical Tips for Clinicians Using Ambient AI to Improve Note Quality and Save Time
Jamie Colbert, MD | Chief Medical Officer
|
March 18, 2026
Ambient AI has the potential to give clinicians something many of us thought we had lost: time.
Time to look patients in the eye instead of the computer screen, to think more carefully about clinical decisions, or to finish a shift without hours of documentation waiting at the end. But like any clinical tool, the value you get from ambient AI depends on how you use it.
As a hospitalist who uses ambient AI regularly, one lesson has become clear: the quality of the note is only as good as the input we provide. It’s not enough to press “record” when you walk into the room and stop when you leave. The best results come when you institute a few minor changes to your workflow to more fully take advantage of the power of ambient AI technology. Here are five simple habits that can dramatically improve the quality, accuracy, and completeness of AI-generated clinical notes.
1. Narrate Your Chart Review
The documentation process doesn’t start when you enter the patient’s room. Before I step inside, I start recording while reviewing the patient’s chart in the EHR. As I scan labs, imaging, and medications, I verbalize the relevant findings.
For example: “Patient admitted with pneumonia. White blood cell count trending down. Chest X-ray shows improving consolidation. Currently on ceftriaxone and azithromycin.”
This helps the AI capture the clinical context—the why behind the visit—before the patient conversation begins. It often produces a stronger HPI and clinical background without any extra work later.
2. Builds Patient Trust with Transparency
Patients are generally curious about the technology when they see it. Even if consent is already documented, I always ask for verbal permission at the start of the encounter and briefly explain what the tool is doing.
Something simple works well: “I use a tool that records our conversation and helps generate my clinical note so I can focus on our conversation instead of typing. Is that okay with you?”
Patients almost always appreciate the explanation. More importantly, they understand why I’m able to maintain eye contact instead of staring at a screen. Transparency turns the technology into a trust-building moment rather than a distraction.
3. Talk Through the Physical Exam
One habit that improves both documentation and patient understanding is thinking out loud during the physical exam. For instance: “Your heart sounds are normal. I’m hearing a little wheezing in the right lower lung.”
This approach accomplishes two things simultaneously. It keeps the patient informed and it gives the AI clear, structured data for the physical exam section of the note. Instead of trying to reconstruct the exam later, the documentation writes itself in real time.
4. Review the Plan in the Room
One of the most common causes of patient messages after discharge is simple confusion about the plan. To prevent this, I walk through the assessment and plan with the patient, and often their family, before the visit ends. Discussing the next steps out loud provides clarity for patients and allows the AI to capture a thorough plan directly from the conversation.
When done well, the plan section of the note is already complete when the visit ends.
5. Capture the “Post-Visit” Thoughts
Sometimes there are elements of clinical reasoning you may prefer not to discuss in detail while the patient is present. In those situations, I simply keep the recording running for about 30 seconds after leaving the room and dictate a quick summary of my thinking.
This brief “brain dump” captures the medical decision-making while it’s still fresh and ensures the cognitive work behind the plan makes it into the note.
Better Input, Better Output
When clinicians first adopt ambient AI, the instinct is to treat it like a passive recorder.
In practice, the technology works best when clinicians actively narrate the clinical encounter. With a few simple habits—verbalizing chart review, explaining findings, and summarizing plans—you can dramatically improve the output while simultaneously enhancing the experience for patients.
Because of these minor changes to my workflow, when I walk out of the exam room the patient is more informed as to their clinical situation and plan of care. And I have a clinical note that is 95% complete. That means less time documenting, and more time face-to-face with my patients.
Most of what drives denials is knowable and fixable, from the front-desk data that starts a claim to the coding and documentation behind it, which is why a structured denial management program pays for itself.
What is denial management?
Denial management is the systematic process of identifying denied claims, finding out why a payer refused them, correcting and resubmitting or appealing them, and fixing the upstream problems so the same denials stop recurring. Done well, it protects cash flow and surfaces the process gaps that cost an organization revenue.
A rejection and a denial aren't the same thing, and the distinction changes how you work each one. A rejection happens before the payer fully processes a claim, usually because of missing or malformed data, so you can correct and resubmit it quickly. A denial happens after the payer adjudicates the claim and decides it won't pay, which means you either correct and resubmit or file a formal appeal.
In medical billing, denial management runs alongside eligibility, coding, and collections, and it depends on all of them, since a claim denied for a coding error or a missing authorization started going wrong long before it reached the payer.
Regulators are responding to the pressure. Under the CMS Interoperability and Prior Authorization Final Rule, impacted payers must, as of January 2026, decide urgent prior authorizations within 72 hours and standard ones within 7 calendar days, give a specific reason for each denial, and publicly report their prior authorization metrics. Those rules should add transparency over time, though the denial volume providers face today is still climbing.
What causes claim denials?
Most denials trace back to a short list of recurring causes across the front end, coding, and documentation. In KFF's analysis of marketplace claims, the single most common reason was an unhelpful "other" category, followed by administrative reasons and excluded services, with lack of prior authorization or referral at 9% and only 6% tied to medical necessity.
In day-to-day billing, the causes that show up most often are:
Eligibility and registration errors, where coverage is inactive or the patient's information is wrong on the date of service.
Missing or incorrect data, from a misspelled name to a transposed member ID.
Missing prior authorization, when a service that needed advance approval didn't get it.
Coding errors, including wrong CPT, ICD-10, or modifier choices, and duplicate claims. Getting this right is where AI medical coding is increasingly earning its keep.
Medical necessity, when the documentation doesn't support the service billed, which ties denial rates directly to clinical documentation improvement.
Timely filing, when a claim lands after the payer's submission window and becomes almost impossible to recover.
Non-covered services and coordination-of-benefits issues, common when a patient carries more than one plan.
Denials also fall into categories that shape how you work them. Soft denials are temporary and can be corrected and resubmitted, while hard denials require a formal appeal or turn into written-off revenue. Administrative denials come from process errors like eligibility or missing data, and clinical denials question medical necessity or coding and need clinical evidence to overturn.
The denial management process, step by step
The denial management process is a repeatable cycle that starts when a payer refuses a claim and ends only when the claim is resolved and the reason behind it is fixed. It breaks into five stages:
Identify and log the denial. Pull every denial from remittance advice, explanation-of-benefits statements, and your payer work queues, and log it right away so nothing slips past the timely-filing deadline.
Categorize the denial. Sort each one by reason code, payer, dollar value, and age, which turns a pile of individual problems into patterns you can act on.
Investigate the root cause. Read the Claim Adjustment Reason Codes and Remittance Advice Remark Codes to understand what actually went wrong, rather than what the denial appears to say on the surface.
Correct and resubmit, or appeal. Fix and resend the claim when it's a correctable error, or build a formal appeal when the payer got it wrong, knowing an appeal can run several rounds of review before it resolves.
Prevent the next one. Feed what you learned back upstream so the same denial stops recurring, which is the stage that compounds over time.
Because about 70% of denials are ultimately overturned once providers pursue them, prioritizing by dollar value, claim age, and likelihood of success is how a team recovers the most revenue with the staff it has.
How to prevent denials
The most effective denial management programs stop denials before submission by tightening the front end, documentation, and coding. Prevention is really about revenue integrity: making sure what's documented, coded, and billed matches the care delivered.
A few practices move the needle most:
Verify eligibility and benefits at registration, so coverage problems surface before the visit rather than after the claim.
Handle prior authorization proactively, tracking which services need it and securing approval early.
Strengthen documentation and coding, since accurate notes and codes are what hold up under payer review. Autonomous coding helps here by generating codes with supporting rationale straight from the documentation.
Capture charges completely, because missed or late charges never surface as denials and become permanent losses, which is why charge capture belongs in any prevention plan.
Track denial trends with analytics, so a spike from one payer or one service line gets caught early.
Build cross-department accountability, matching each denial type to the team that can prevent it, from front desk to coding to billing.
Platforms like Commure Pro pull coding, charge capture, and documentation into one layer so these controls run on every encounter instead of depending on someone remembering to check.
Metrics that matter in denial management
A handful of KPIs tell you whether your denial management is working. The core four are your denial rate (the share of claims denied), your appeal overturn rate (how often you win the denials you fight), your days to resolution (how long a denial takes to clear), and your write-off rate (the revenue you give up).
There's no universal target, but recent MGMA benchmarking put the aggregate first-pass denial rate near 8%, and many organizations run well above that. Two other numbers frame the opportunity: denials get overturned roughly 70% of the time when pursued, and each one costs about $57.23 to work, so a lower denial rate and a higher first-pass yield translate directly into recovered margin.
How AI is changing denial management
AI is shifting denial management from an after-the-fact cleanup job toward prevention, flagging at-risk claims before they're submitted, and automating the appeals and resubmissions that used to consume staff hours. The same models can categorize denials by reason code, group similar claims for bulk resubmission, and draft appeals with the supporting documentation attached.
That's the approach behind Commure's AI work on denials, which pairs accurate coding and charge reconciliation on the front end with automated denial categorization and resubmission on the back end. One New York health system cut its timely-filing denials by 53% and raised monthly charges by 20% (from $7.5M to $9.4M) after deploying automated charge note reconciliation, detailed in the NYC health system case study.
Denials are one piece of a broader move toward healthcare automation across the revenue cycle, where prevention on every claim beats recovery on the ones that slip through.
Turning denial management into prevention
Denial management works best as part of a connected revenue cycle, where clean documentation, accurate coding, and complete charge capture combine into a claim that's right the first time. That's what revenue cycle management built on AI is meant to deliver.
See how Commure RCM turns denial management from a recovery scramble into a prevention system.
What is the difference between a claim denial and a claim rejection?
A claim rejection happens before the payer processes the claim, usually because of missing or invalid data, so you can correct and resubmit it quickly. A denial happens after the payer adjudicates the claim and refuses to pay, which means you either fix and resubmit it or file a formal appeal. Rejections clear faster; denials take more work.
In medical billing, denial management is the workflow billing teams use to catch, correct, appeal, and prevent denied claims. It covers reading payer reason codes, resubmitting fixable errors, appealing wrongful denials before filing deadlines close, and feeding root causes back to registration, coding, and documentation so the same denials stop recurring.
What are denial management services?
Denial management services are the people, software, or outsourced partners that handle denied claims for a provider. They range from in-house billing teams to third-party RCM vendors and AI-driven tools that flag at-risk claims before submission, categorize denials by reason code, and automate resubmissions and appeals to recover revenue faster.
What is the difference between denial management and revenue cycle management?
Denial management is one part of revenue cycle management, which covers the full financial path of a claim from registration and eligibility through coding, billing, and payment posting. Denial management focuses specifically on the claims a payer refuses, resolving them and preventing the next ones, so it only works as well as the revenue cycle around it.
If you've spent any time in home health care operations, you already know the math: the agency that responds first wins the patient. It doesn't matter how good your clinical team is or how strong your outcomes are, if you're still processing referrals through fax queues and manual spreadsheets, you're losing business to the agency that picked up faster.
Referral intake is the front door to your entire business, and right now, for most agencies, that front door is held together with fax paper. 75% of home health organizations still rely on fax as their primary referral channel. Home health industry estimates 10 minutes per referral, scaling to five to eight hours of administrative time weekly at 30-50 referrals per week. Despite that investment, only 50% of referrals convert on average
Payers, hospitals, and discharge teams aren't waiting around. They're sending the same referral to a dozen agencies simultaneously, and they're moving on quickly. When your intake team is manually keying demographics, chasing payer verification, and managing status updates across phone calls and portals, you're leaving revenue on the table.
The administrative burden doesn't just cost agencies with missed referrals. It costs staff. The volume of manual, repetitive work in referral intake is one of the leading drivers of burnout and turnover on intake teams, a problem that compounds itself as agencies struggle to backfill.
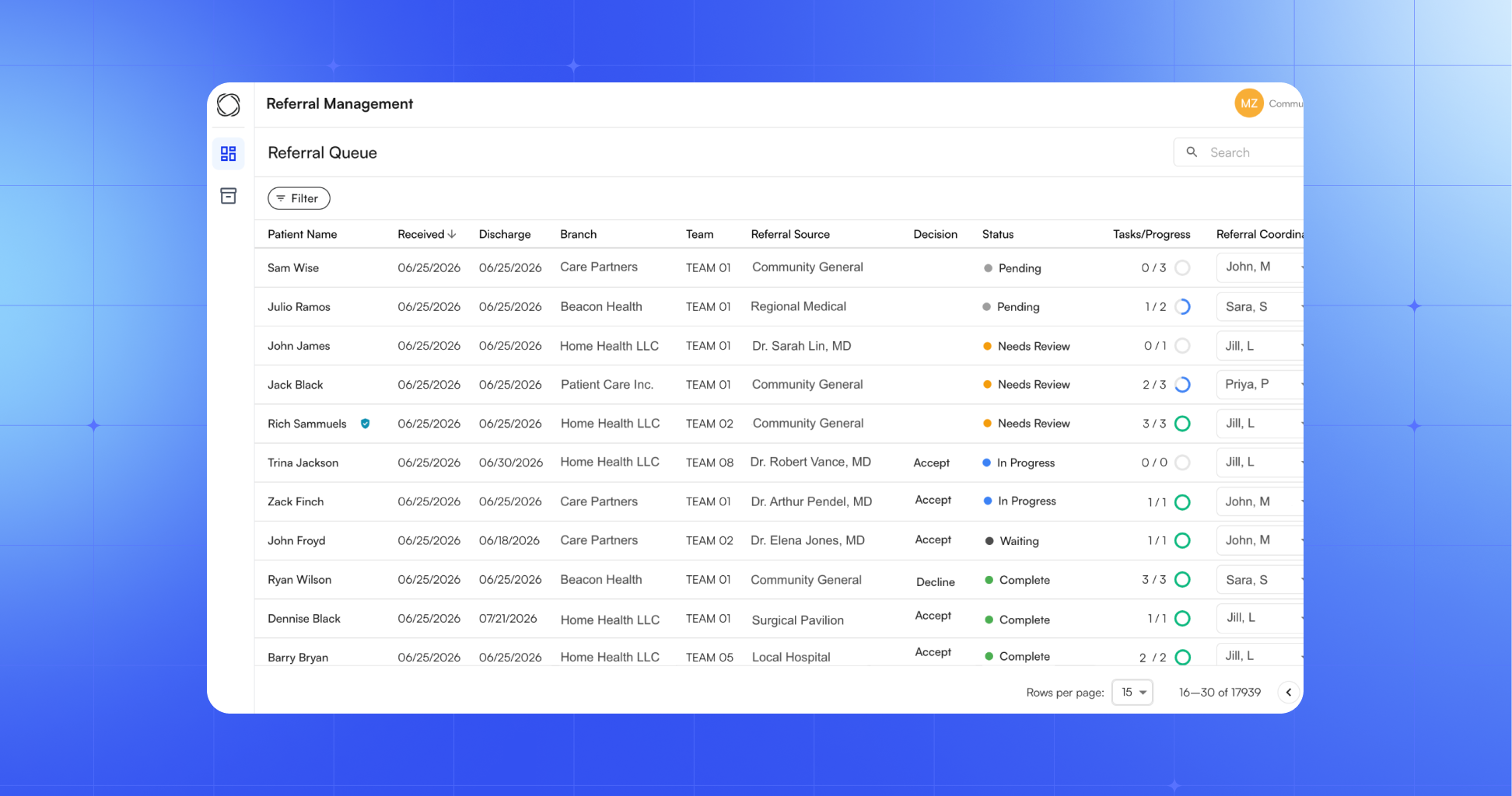
Introducing Commure Orchestrator for Home Health
Commure Orchestrator is an AI-native referral management platform that automates the entire intake workflow, from the moment a referral arrives to the moment a patient is admitted. No manual handoffs, dropped follow-ups, or data entry.
The platform operates across five automated steps:
Ingest. Referrals are captured from every source the moment they arrive (fax, portal, EHR, email) and pulled into a single unified system. Your team stops chasing down incoming referrals across channels and starts working them.
Extract. AI automatically structures every referral: patient demographics, clinical notes, payer information, diagnosis codes. The data is clean, complete, and ready to act on, without anyone retyping it.
Validate. Every business rule your agency runs, including service area, acuity, and payer eligibility, executes automatically before anyone touches the referral. Manual checklist work disappears.
Coordinate. One queue for every team. Communication is centralized so there are no emails, spreadsheets, or dropped handoffs between intake, clinical, and scheduling staff.
Close. Accepted referrals write directly back into the EHR. The audit loop closes automatically. Zero manual data entry at the back end.
The result is faster response times, higher acceptance rates, and a meaningful reduction in the administrative load your team carries every day.
One Workflow. Impact Across the Organization.
The effects of a faster, more automated intake process compound across the business:
Revenue: Reduce missed referrals with higher acceptance rates.
Operations: Increase staff throughput without adding headcount.
Patient experience: Reduce time-to-care by matching patients to available capacity faster.
Compliance: Maintain audit-ready, real-time visibility across your entire referral pipeline.
Commure Orchestrator integrates with AI Call Center Agents and digital patient intake, so automation doesn't stop at intake approval. Once a referral is accepted, patients can be scheduled immediately, and pre-visit intake can be completed via SMS or email before the first visit, connecting the full referral-to-visit handoff without gaps.
Orchestrator is already processing hundreds of thousands of tasks fully autonomously across home health, ambulatory, and specialty care settings.
Ready to See It in Action?
If your intake team is still managing referrals manually, we'd like to show you what a fully automated workflow looks like in practice.
Before we built Patient360, my team and I spent weeks shadowing providers across hospitals and ambulatory clinics. The pattern was hard to miss: providers were spending 10 to 20 minutes prepping for a patient they'd see for 5 or 10 minutes.
And that prep time wasn't spent thinking about the patient. It was clicking through the EHR, pulling up labs and imaging one screen at a time, and calling around to track down documents that never made it into the chart.
Tens of thousands of providers now use it to walk into visits already caught up; this post is about what they've taught us so far.
The medical note was only half the problem
Commure Ambient AI solved clinical documentation. Providers stopped working on documentation at 10 pm and are now finishing their notes within a few minutes.
But when we asked providers where their remaining time was going, they pointed to everything that happens before the visit. Documentation had gotten faster while prep was still as slow as it had always been.
Providers didn't go to medical school to click through 20 screens collecting information. They went to make judgments and care for patients. Our job at Commure is to synthesize everything and hand it to them so they can do exactly that.
So we started building beyond the note. Patient360 is a complete clinical picture of the patient, assembled continuously from EHR data: labs, imaging, medications, allergies, signed notes, and past appointments.
That picture powers two things providers touch every day. The first is an AI pre-visit summary that gets a provider current on a patient in about 60 seconds, tailored to their specialty. The second is an AI assistant that answers natural-language questions about the chart, like "any abnormal labs since the last visit?"
Specialty tailoring was a day-one decision. A cardiologist and an orthopedic surgeon need different labs, different baselines, and different acronyms, so a generic summary gets you 60% of the way, which still leaves the provider digging through the EHR to close the gap. With insights from specialists working in the field every day, we created specialty-specific summaries for cardiology, orthopedics, oncology, OBGYN, and more.
"Patient360 gave me exactly what I needed to prep for the visit — the right level of patient-centered information, surfaced at the right time. The reminders on incomplete tests were especially valuable. We've been extremely pleased with the pre-visit summary." — Kansas Heart
What providers have taught us so far
The most common feedback in our early rollouts was a request for more. Providers who had the summary and assistant before the visit asked if they could have access to the tools during and after the visit as well.
The second lesson was how dramatically prep timing shifts once the work is done for you. One clinical practice told us they used to prep charts a full week ahead because the process took so long. Now their providers review the summary 2 minutes before walking in.
"Patient360 has been extremely helpful. Yesterday, with a busy clinic schedule and an eval about to start, I used it to quickly get the key context for the visit. It gave me exactly the information I needed and saved me several minutes of going into the chart to find the information." — Athens Orthopedics
The third surprised me. Some care teams included Patient360 as part of their daily huddle, pulling it up so everyone's current on a patient in seconds before discussing the case. We built it for individual prep, and providers turned it into a collaboration tool.
And the fourth is my favorite. Providers who had been hesitant about recording visits at all loved Patient360 once they saw what it gave them in return.
"Seeing providers who are typically slower to adopt new technology quickly embrace Commure, and specifically Patient360, has been a huge win. They're using it daily to prepare for visits faster and review patient information more efficiently. Now we want to see it rolled out across the entire site." — Mountainlands Community Health Center
Trust is everything
Every enterprise conversation I have starts with some version of the same question: how do I know the data is correct and safe?
It's the right question. A summary that's wrong, or that omits something like a prior heart attack, can be nearly as harmful as the EHR chaos it replaced. Trust in healthcare AI has to be earned in the product itself, so we built it with trust as the leading factor from the start.
Every insight in Patient360 links back to its source in the chart. If a provider wants to verify where a statement came from, the citation is one click away.
And when the chart conflicts with itself (which happens constantly when different providers document different things), instead of picking a winner, we surface the conflict on the summary so the clinician can make the call with full information.
What providers consistently asked us
Across these first rollouts, providers and health system leaders kept pressing us on the same three questions. They're the right ones to ask of any tool in this space.
Can I trust the data? They asked how we handle conflicting information, whether every insight is cited to its source, and how we think about what's missing, since an absent heart attack is nearly as dangerous as an invented one.
Does it fit the workflow I already have? The worst outcome is a tool providers have to learn. Patient360 was built alongside clinicians from the first design review, and our bar is zero-second training: you open it, and you're ready.
Where Patient360 goes next
Patient360 started as the picture a provider sees before the visit. It's becoming the insights layer underneath the whole encounter.
Pre-charting is next: Patient360 context will flow directly into the medical note, so relevant history, labs, and the HPI foundation are already in place before the provider enters the room and starts documenting the encounter. We're also ingesting the documents and detailed medical history that live as PDFs in the chart, like scanned imaging results and referral packets, so nothing gets left out of the picture.
After that comes in-visit intelligence: care suggestions that surface in real time as the conversation unfolds, always as options the provider can accept or dismiss, never decisions made on their behalf.
Our goal is the same one we started with. Providers should spend their training and judgment on patients, and Patient360 exists to clear away everything standing in between.
If your team is still prepping charts a week in advance, come see what a 2-minute prep workflow actually looks like. Email us at solutions@commure.com or book a demo via the button below.
Healthcare automation has already saved the US health system hundreds of billions of dollars. Electronic transactions and automation helped the industry avoid an estimated $258 billion in administrative costs in 2024, with roughly $21 billion a year still available from work that stays manual or partly manual, according to the 2025 CAQH Index.
The strain behind those figures shows up on every clinical schedule. Physicians reported a 57.8-hour workweek in 2024, and 7.3 hours of it went to administrative tasks like prior authorization, insurance forms, and meetings, per the American Medical Association.
For health systems looking to cut administrative costs and give staff time back, the real question is what to automate, in what order, and how to do it without adding risk.
What is healthcare automation?
Healthcare automation is the use of technology to complete healthcare tasks with little or no manual effort, across operational, financial, and clinical work. It covers everything from insurance eligibility checks and claims processing to clinical documentation and patient reminders.
Most people first meet it in its narrow form, robotic process automation (RPA) in healthcare, where software handles repetitive, rule-based steps such as data entry or eligibility verification. The broader term is intelligent automation, which combines RPA with artificial intelligence so systems can read unstructured documents, interpret context, and make complex decisions.
Health care automation works best when it runs across a whole process rather than one isolated step, so a patient's information moves from intake through documentation, coding, billing, and follow-up without being re-keyed at each stage.
The main types of healthcare automation
Healthcare automation spans a few distinct technologies, and knowing the difference helps you match the right tool to the right job.
Robotic process automation (RPA). Software bots follow fixed rules to handle high-volume, repetitive tasks like eligibility checks, claim status lookups, and moving data between systems. It's fast and reliable for work that never changes.
AI and machine learning. These models find patterns in data, so they can predict likely claim denials, prioritize worklists, or surface a possible diagnosis for clinician review. They get better as they see more examples.
Intelligent automation. This pairs RPA with AI so a single workflow can read a faxed referral, pull the relevant clinical details, and route the case, handling the messy inputs that rule-based bots alone can't.
Ambient AI. Ambient AI listens during a visit and drafts the clinical note in real time, which is why teams often ask how ambient AI and AI scribes differ. It takes documentation off the clinician's plate entirely.
Agentic AI. The newest layer, agentic AI, can plan and carry out multi-step tasks on its own, check its work against policy, and pull in a human when a case needs judgment.
You don't have to pick just one. Most decisions here land with the people accountable for operations, revenue, and IT, so whether you're a COO weighing throughput, a revenue cycle or finance leader watching cost per claim, or a CMIO protecting clinician time, the goal is the same. A mature program uses all of these types, matched to the risk and complexity of each task.
Where healthcare automation works across health systems
Healthcare automation can be applied across the entire care and revenue journey, not only the billing office. Health systems get the most from it when their automation connects these areas, so information flows from one to the next instead of stopping at department lines.
Patient access and intake. Automated scheduling, reminders, and digital intake reduce no-shows and cut front-desk phone volume, while eligibility checks confirm coverage before the visit. This is the front end of patient engagement, where modern patient communication software handles two-way conversations: reminders, replies, scheduling, and follow-up in one place. Yale New Haven Health used automated pre-visit outreach to cut no-shows and same-day cancellations by 54% in its breast imaging program.
Clinical documentation. Ambient AI drafts notes during the encounter, and dictation feeds structured data back into downstream systems, so clinicians spend less of the visit typing.
Patient communication and coordination. Healthcare AI agents handle inbound calls, answer routine questions, and manage follow-up, freeing staff for work that needs a human.
Back office. Supply chain ordering, compliance reporting, and security monitoring all run more accurately when automated systems handle the routine checks.
The core benefit of healthcare automation is time returned to people, which then shows up as lower costs, fewer errors, and a better experience for patients and staff.
When automation absorbs data entry, paperwork, and documentation, clinical teams spend more of the day on care and administrative teams move to higher-value work. At North East Medical Services, clinicians started heading home 1 to 2 hours earlier each day after adopting ambient AI.
Costs also drop and revenue holds. Fewer manual touches mean fewer coding and billing errors, faster payment, and less rework, which is how one New York City health system raised revenue cycle performance by 20%.
Patients notice too. Faster scheduling, quicker responses, and fewer forms make the experience smoother, and automated follow-up keeps people engaged between visits.
Automation also scales in a way that hiring can't. A system absorbs higher patient volumes without adding headcount for every task, and automated access controls and audit trails support compliance along the way.
What to automate first
Start where the burden is heaviest, and the payoff is fastest to see, then expand into adjacent work. Early, visible wins build trust that carries into the next project.
Clinical documentation is the clearest first move. It's the single largest source of clinician time and burnout, and ambient AI addresses it directly by drafting the note during the visit for the clinician to review and sign, so results show up right away in reclaimed hours and less after-hours charting. Because a clinician still approves every note, the clinical risk stays low while the relief is immediate.
Prior authorization is the next obvious candidate. Physicians and their staff spend about 13 hours a week on it, completing roughly 40 requests per physician, and 40% of practices now employ people who work on nothing else, according to the AMA's 2025 survey. It's high volume, highly repetitive, and directly measurable, which is exactly the profile automation handles well.
Eligibility verification, patient intake, claim scrubbing, and appointment reminders fit the same criteria and are common early wins.
Sequence matters as much as selection. Prove the value on one workflow, measure the time and money it returns, then expand into adjacent steps. A phased rollout produces the hard numbers you need to justify each next investment.
Why healthcare automation succeeds or stalls
Automation succeeds when it fits how clinicians already work, and it stalls when it's bolted on without their input. The technology is rarely the hard part; adoption is. A few practices separate the programs that stick from the ones that stall:
Bring staff in early. Involve the clinical and administrative teams who'll use the tools before you buy, so the workflow fits their day instead of fighting it.
Aim for top-of-license work. Target the tasks that pull people away from what they trained for, and measure success by the time given back, not screens added.
Keep a human in the loop. Let automation handle the routine work and route exceptions and anything with clinical or financial weight to a person for review.
Start small and prove it. Roll out one workflow, show the time and dollars it returns, then use those numbers to justify the next phase.
Get governance right from day one. Automated systems touch protected health information, so insist on HIPAA-compliant handling, clear audit trails, and attention to model bias.
Integrate with the EHR. Tight integration keeps data accurate and stops staff from re-keying information between systems.
Healthcare automation is now core infrastructure
Healthcare automation is no longer optional: health systems and mid-sized practice groups nationwide are treating it as a core part of how they operate and compete. The organizations seeing the greatest results treat it as one connected system, starting where the work is most repetitive and the ROI is hardest to ignore. The real opportunity lies in building automation that compounds, with each layer making the next one more powerful.
See how the Commure platform brings ambient AI, revenue cycle, and patient engagement together in one place.
Frequently asked questions
What are examples of healthcare automation?
Common examples include automated appointment scheduling and reminders, insurance eligibility checks, medical coding, claims processing and denial prevention, ambient AI that drafts clinical notes, and AI agents that handle patient phone calls. More than 50% of health plans and 25% of provider organizations now use AI in administrative workflows, per the 2025 CAQH Index.
What's the difference between RPA and AI in healthcare?
RPA follows fixed rules to automate repetitive tasks like data entry and eligibility checks, and it can't adapt on its own. AI uses machine learning to interpret data, predict outcomes, and handle unstructured inputs like faxed referrals. Intelligent automation combines the two, which is what most healthcare workflows actually need.
Will healthcare automation replace healthcare jobs?
No. Healthcare automation mainly targets administrative and repetitive work rather than clinical judgment, so it shifts staff toward higher-value tasks instead of eliminating roles. Physicians spend 7.3 hours a week on administrative tasks alone, per the AMA, and automating that work lets clinical teams operate at the top of their license.
Is healthcare automation HIPAA compliant?
It can be, when built correctly. Automation tools handle protected health information, so they need HIPAA-compliant data handling, encryption, access controls, and audit trails. Compliance depends on the vendor and configuration, not the technology itself. Commure is HIPAA-compliant and built for enterprise health systems, so hold any platform you evaluate to that same standard.
How do you get started with healthcare automation?
Start with one high-volume, rule-based, low-risk workflow such as prior authorization or eligibility verification. Measure the time and money it returns, then expand into adjacent steps. A phased rollout builds staff trust and produces the hard numbers you need to justify each next investment.
Tell us a little bit about yourself—what do you like to do outside of work?
Relocating from Long Island, NY, 5 years ago with my wife and 2 daughters, ages 8 and 6, to the Raleigh-Durham, NC area - there is no shortage of fun to keep us busy down here. From hiking trails at the lake to pickleball to dance class to the swim team, we are always keeping active. My daughters are slowly becoming “foodies” too. They don’t run with the chicken nugget and tater tot crowd. They love sushi and ramen. They love “millionaire” bacon (just add a little brown sugar) and “fruity-face” pancakes. We grill year-round - my kids are carnivores! - so my rib-eye steak and cheeseburger game is on point. North Carolina is known for its BBQ - we’ve tried many of the local places and think we found our go-to spot. We have also started baking together more - the kitchen gets wrecked, but we have a blast, and the end product is always worth it. Look up the recipe for Hummingbird Cake and thank me later.
As a kid, what did you want to be when you grew up?
I thought I wanted to be a doctor - then I took Organic Chemistry in college as a Pre-Med major…that's when I learned I didn’t really want to be a doctor. Whenever my kids need a band-aid, I’m quick to tell them: “Don’t worry, Dad was pre-med for a semester. You’re in good hands.”
I wound up studying Psychology and Sociology at the University of Notre Dame (Go Irish!), with intentions to pursue a career as a Sports Psychologist - but upon graduating instead received a wonderful opportunity in the Real Estate and Construction sector back home in New York City. This role afforded me an opportunity to work on many high-profile projects - many of which were engagements with large health systems such as NYU Langone Medical Center, Memorial Sloan Kettering, and Mount Sinai. My company at the time leveraged proprietary VR/AR software to design, manufacture, and build sustainable medical care spaces - everything from hospital headwalls and footwalls with embedded medical gases to millwork for nursing stations.
Describe a day in the life of your role.
As an Account Manager, serving as the single point of contact for our partners - the role touches every phase of every product in our bundle. A typical day looks like this: execute on whatever it is your partners require. We are full-time client advocates, relationship managers, issue-resolvers, account retainers, project coordinators, revenue and data analysts, product experts, process/workflow builders, strategic consultants, and often…behavioral psychologists!
What made you decide to join Commure?
From my time in construction, I learned this: demolition is easy; building is hard. Anybody can tear down or point out faults. The real skill and true craftsmanship is reserved for the creators and builders - people who take empty space and transform it into something beautiful and useful. Good design is both form and function, in harmony - the Commure product suite nails this.
Seeing firsthand the significant impact Real Estate and Facilities projects have on patient care - and a medical practice’s ability to generate revenue - laid the groundwork for pursuing a role at Commure to tackle the healthcare problem. The United States is #1 in the world in wealth, but outside the top 30 in healthcare delivery - this needs to change.
How would you describe the Commure company culture?
This is a team sport. While we each have distinct responsibilities, we operate as one team. Our culture is defined by collaboration, accountability, and a relentless focus on client outcomes. Across the organization, we are united by a common mission: building best-in-class, AI-native products to improve provider productivity, reduce administrative burden, and allow healthcare teams to focus on what matters most - patient care.
What advice would you give someone on their first day at Commure?
Be a heat-seeking missile for pain - actively seek the gnarliest challenges and pain points that impact our customers. Prioritize building product knowledge and expertise across our bundle. Operate without fear. Dive headfirst into ambiguous challenges, and when you identify a gap - the standing order to my team - go bridge the gap. You do not need to ask permission. Brick-by-brick, drive the company forward.
What has been your greatest accomplishment so far at Commure?
We have accomplished so much in my 2+ years - improving user experience while surfacing inconsistencies in claims before they were submitted - and fixing claims we knew an insurance company would deny payment before they were submitted. The impact of this release was astonishing - automating previously time-consuming workflows while improving First Pass Rate and cash flow for partners across our portfolio.
What does "a win" look like in your role?
Earning a renewal and extending into a multi-year partnership. It shows we have built trust, delivered meaningful results, and created an experience that our partners want to continue investing in. Those outcomes only happen when all disciplines - including Sales, Launch, Account Management, Operations, Engineering, Product, and Support - are working in harmony - one team. Every renewal strengthens our business and expands our opportunity to improve healthcare for more patients and providers.
Interested in a career building the next generation of healthcare technology powered by AI? We are always looking for talented people across our departments.
A new patient in one of the 15 largest metro areas in the U.S. now waits an average of 31 days to see a physician, according to AMN Healthcare's 2025 survey, and rural patients often wait longer still (roughly 20% of Americans live in rural areas while only about 9% of physicians practice there, according to the National Rural Health Association). That wait is a symptom of a system that loses patients before the patient journey ever begins, and every day of delay is a chance for someone to switch providers, defer care, or disappear from the schedule entirely.
The patient journey is the full arc of a person's experience with a health system, from the first symptom or online search, through treatment and long-term follow-up. Health systems have mapped that journey for years, yet far fewer have fixed the gaps along the way.
This guide covers what the patient journey is, the stages every patient moves through, how to map it, and how to close the gaps that quietly cost health systems patients and revenue.
What is the patient journey?
The patient journey is the sequence of interactions a person has with a healthcare organization over time, starting well before a first appointment and continuing long after a visit ends. It covers how someone finds a provider, books and prepares for care, moves through the visit itself, and stays connected for follow-up and ongoing needs.
Much of the healthcare patient journey plays out beyond the exam room: the phone tree at scheduling, the intake form, the reminder that does or doesn't arrive, the call after a procedure when a question comes up at 9 p.m.
It helps to separate two terms that often get used interchangeably. The patient journey is what actually happens to the patient. A patient journey map is the tool you build to see that experience clearly and decide what to change.
Why the patient journey matters
Healthcare has shifted from a system patients accepted to one they shop, and people now compare providers the way they compare any other service. That shift shows up plainly in switching behavior. About 1 in 5 patients switched providers in the past year, and nearly 90% of them did so because the organization was hard to do business with, according to an Accenture survey reported by the American Hospital Association. 7 in 10 pointed to access as a deciding factor when they chose someone new.
That pattern points squarely at the friction around care: the busy phone line, the confusing bill, the message that never gets a reply. Every one of those friction points sits somewhere on the patient journey, which is why mapping it and fixing what you find has become a retention strategy in its own right.
The stages of the patient journey
Most patient journeys move through 6 stages: awareness, consideration, access, the visit, follow-up, and ongoing care. Few patients travel them in a tidy line, since people loop back, pause, or drop out along the way, but the stages give you a shared structure for pinpointing where the experience breaks down.
Awareness
Awareness starts the moment someone notices a symptom or decides they need care. Most people begin with a search engine rather than a physician referral, so the clarity of what they find shapes their first impression of your organization long before they ever call. Content that answers real questions, a findable location listing, and current reviews all work well at this stage.
Consideration
In the consideration stage, patients weigh their options against practical criteria: location, accepted insurance, reviews, and whether they can actually reach you. This is where many patients silently choose a competitor, often for reasons that have nothing to do with clinical quality. A booking page that asks for too much, a call that goes to voicemail, or a week-long callback delay can end the relationship before it begins.
Access
Access is where the journey stalls more often than not. With new-patient waits averaging a month across major metros, the organizations that win patients are the ones that make scheduling fast and answer the phone reliably.
Access is also one of the more fixable stages. One community health center that began handling inbound calls with AI call center agents saved 800 labor hours for every 10,000 calls, roughly $240,000 a year, while resolving a large share of requests without staff involvement. Widening patient access at the front door keeps patients from giving up before they arrive.
Preparation belongs to this stage too. Long paper forms and prep instructions that are easy to miss create no-shows and day-of delays, which is why modern patient intake moves the clipboard onto the patient's phone through conversational outreach. Timely, multi-touch reminders that patients can actually respond to help reduce no-shows and protect both the schedule and the revenue attached to it.
The visit
The visit is where clinical care happens and where traditional patient-satisfaction measurement concentrates, spanning check-in, the encounter, and discharge. It's also where communication gaps take root, since patients often leave without asking the questions that mattered most to them and forget a large share of what they were told once they get home. What happens over the following days depends heavily on how well the visit sets them up.
Follow-up
Follow-up is the stage health systems most often let slide, even though it's where good clinical work can come undone. A 2026 study of more than 579,000 Medicare admissions found that many high-risk patients never receive post-discharge follow-up, and those who did were significantly less likely to be readmitted within 30 days. After a procedure, patients navigate medication questions, recovery uncertainty, and handoffs between care teams, and every handoff is a point where someone can slip through the cracks.
Two strategies make a measurable difference here. Tighter transitions of care keep information from getting dropped as a patient moves between settings, and proactive outreach closes the post-surgical care gap during the window when patients are home and most likely to need answers.
Ongoing care
Ongoing care turns a single visit into a lasting relationship that supports better health. For someone managing a chronic condition, this stage can stretch across years, and it's where loyalty is either earned or lost. Steady, personalized chronic care management keeps patients engaged between appointments, surfaces problems earlier, and reduces the avoidable complications that pull people back into acute care.
Patient journey mapping
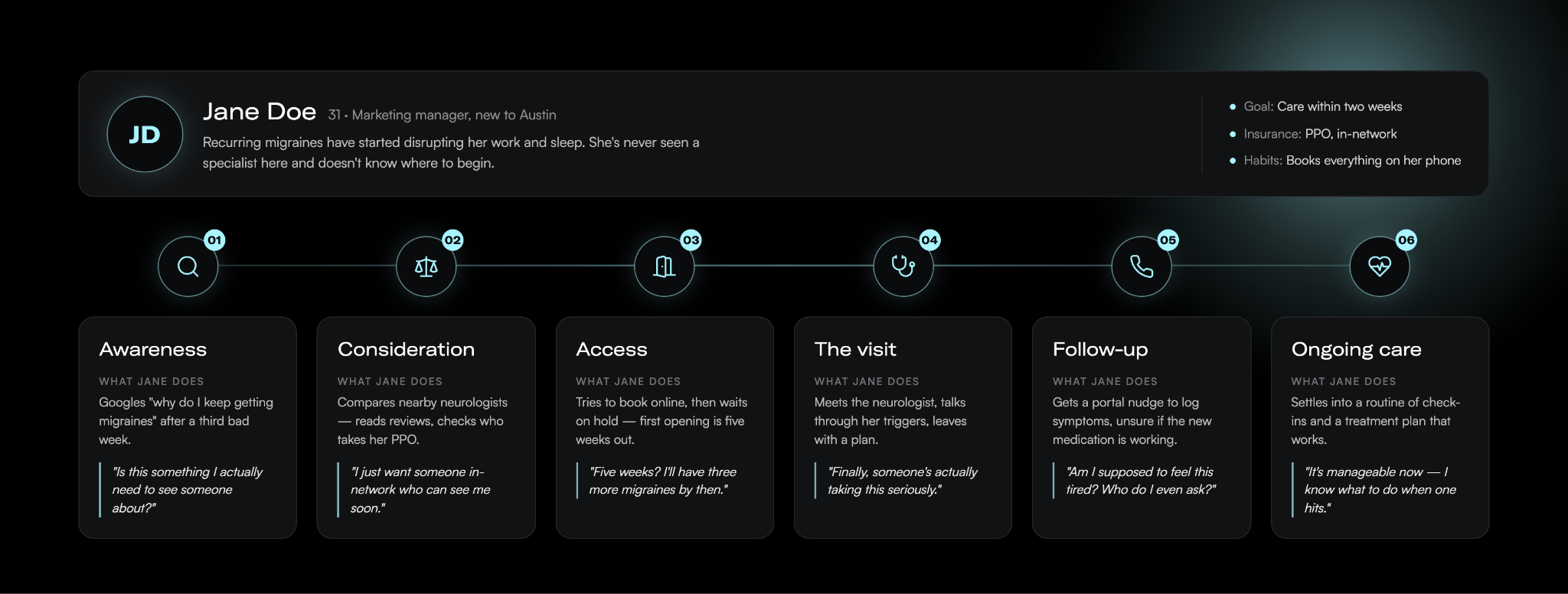
Patient journey mapping is the practice of laying out each stage, touchpoint, and emotion a patient experiences, so you can see where the journey serves them and where it fails them. The patient journey map is the visual result, a shared picture of what patients do, think, and feel as they move through your system.
Here is a very basic example of a patient journey map. The more details you can fill in, the better.
Done well, a map earns its keep in a few ways. It creates a common view of the experience across departments that rarely talk to each other, exposes the specific moments where patients get stuck, and turns vague complaints about "patient experience" into a prioritized list of fixable problems.
Types of patient journey maps
Teams generally build one of four map types depending on the question they're answering.
A current-state map shows the journey as it runs today, drawn from real patient data, and it's the right starting point for incremental improvement.
A future-state map describes the journey you want to deliver and works well for aligning teams around a new service or process.
A day-in-the-life map widens the lens to what a patient experiences outside your system, which helps you spot unmet needs you'd otherwise miss.
A service blueprint goes the other direction and adds the people, systems, and policies behind each touchpoint, so you can trace a pain point back to the process that caused it.
Most organizations start with one type and add others as the work matures.
Patient journey analytics
The strongest maps sit on data. Patient journey analytics is the practice of layering your operational and experience data onto the map: scheduling and no-show records, call-center hold times, message response rates, portal usage, and post-visit feedback. Those numbers show you where patients actually drop off rather than where you assume they do, and they let you measure whether a change at one touchpoint moved the outcome you cared about.
How to map the patient journey
Here are the steps to take to build out your patient journey map:
Define your scope and goal. A map can zoom in on a single interaction, like booking an appointment, or span an entire condition, like managing diabetes over several years. Let the problem you're trying to solve set the boundaries.
Gather data from multiple sources. Combine direct patient input from interviews, surveys, and short diary studies with the operational and experience data you already hold, like scheduling records, message response rates, and existing patient satisfaction and engagement survey scores. Interviews add depth, surveys validate patterns at scale, and the data you already collect grounds the whole map in what really happens.
Build personas. A new mother's journey looks nothing like an oncology patient's, so segment by the populations you actually serve rather than mapping a generic average patient.
Chart touchpoints and emotions. For each stage, record what the patient does, who and what they interact with, and how they feel. The emotional low points usually mark your biggest opportunities, since that's where frustration leads to a decision to leave.
Validate and act. Put the draft in front of patients and frontline staff to catch what you missed, then commit to fixing the touchpoints it exposes. A map only pays off when it drives real changes to how you operate.
Common mapping mistakes
A few mistakes hurt the value of patient journey mapping. The most common is treating the finished map as the deliverable, when the map only matters once it changes how you work. Others include mapping the journey your organization wishes patients took instead of the one they actually take, building the whole thing from internal assumptions without talking to a single patient, and mapping so broadly that no team owns any specific fix. Assigning clear ownership for each stage, and revisiting the map as your services and patients change, keeps it from going stale.
Closing the gaps
Finding the gaps is the easy part; closing them, stage by stage, is where patient experience actually improves and where retention follows.
In practice, that means answering the phone during the access stage, replacing paper intake with conversational outreach before the visit, and staying in contact through follow-up and ongoing care instead of going quiet once the encounter ends. The connected set of tools that supports patients across all of these stages is what many health system leaders now call the digital front door, and it works best as a single platform that writes back to the EHR rather than a stack of disconnected point solutions. Keeping patients informed between visits is the job of patient communication software that reads each reply and routes anything a human needs to handle to the right person.
Commure Engage is built for exactly this work, supporting front-cycle patient experience across scheduling, intake, communication, and care navigation on one platform. Yale New Haven Health used Commure Engage for pre-appointment outreach in its breast imaging program and cut no-show and same-day cancellation rates by more than half.
Map the journey your patients actually take, then close the gaps one stage at a time. See how it all comes together.
What is the difference between the patient journey and the patient experience?
The patient journey is the full sequence of steps a patient moves through, from first symptom to ongoing care. The patient experience is how they perceive and feel about those steps. The journey is the path, and the experience is the quality of each interaction along it, which is why you map the journey to improve the experience.
What are the stages of the patient journey?
The patient journey typically moves through 6 stages: awareness, when someone notices a symptom; consideration, when they weigh providers; access, when they schedule and prepare; the visit, when care happens; follow-up, after a procedure or discharge; and ongoing care, which sustains the relationship over time. Few patients travel them in a straight line.
Who is responsible for the patient journey in a health system?
No single department owns the patient journey, which is part of what makes it hard to fix. It crosses scheduling, front-desk staff, clinicians, billing, marketing, and IT, so improving it takes shared ownership rather than one team's effort. Most organizations assign an owner for each stage plus a cross-functional group to keep the full journey aligned.
How can health systems improve the patient journey?
Health systems improve the patient journey by fixing the touchpoints a journey map exposes, stage by stage. The biggest gains usually come at access: answering the phone, offering online self-scheduling, and replacing paper intake with digital outreach. A July 2025 MGMA poll found 71% of practices have less than 25% of their patients using digital tools to self-schedule, so the opportunity is wide open.
When a clinic reaches a patient by phone before a visit, only 3% miss the appointment. When the reminder lands in voicemail, that climbs to 24%. When no one picks up at all, 39% don't show. Those numbers come from a study of 250 primary care patients managing depression, published in Psychiatric Services, and they point to something most communication tools get wrong. Reaching a patient and sending a message are two different things.
For 20 years, patient communication software has mostly meant reminders. An appointment gets booked, the system fires off a text or a robocall, and the office hopes it lands.
Modern patient communication software works differently. It's two-way, omnichannel, automated, HIPAA-compliant, and EHR-integrated. Instead of sending a text and hoping the patient receives it, AI reads each patient's reply, responds in natural language, and routes anything that needs a human to the right person.
Why one-way reminders hit a wall
Reminders work, up to a point. A randomized trial published in AJMC tested three approaches: a reminder 3 days out, 1 day out, or both. Patients who got both missed 4.4% of appointments, compared with 5.8% and 5.3% for a single reminder 3 days or 1 day before.
In that same research, the highest-risk group still missed roughly 20% of visits even after two reminders. The authors concluded automated messages have to be backed by staff outreach or patient navigation to engage with those patients.
So the old model forces a hard choice. Send more reminders that high-risk patients already skip, or put staff back on the phones.
A modern patient communication platform closes that gap. Automated digital care pathways are personalized to patients' unique care journeys, and AI call center agents can handle the follow-up calls that used to eat staff hours. One FQHC saw its agents save 800 labor hours for every 10,000 calls, about $240,000 a year.
What modern patient communication software actually does
Modern platforms respond, instead of just sending. When a patient texts a question, AI reads the reply and answers in plain language, drawing on a clinician-curated knowledge base, so responses stay inside vetted clinical boundaries. Anything urgent, or anything the system shouldn't answer on its own, routes to the right care team member.
None of this requires a portal login or an app. The platform reaches patients by SMS, RCS, voice, or email, and every exchange writes back to the EHR so the care team sees it where they already work.
Routine outreach runs on its own. Appointment prep, reminders, and post-visit check-ins go out automatically, without staff sending them one by one. The result is one continuous conversation with each patient instead of a scatter of one-way pings.
How to evaluate patient communication software
When you compare platforms, four things separate one that works from one that adds cost. Here’s what to ask when comparing vendors:
Ask whether it's genuinely two-way and omnichannel. A tool that only pushes messages out is a reminder system with a new name, and it leaves you managing the same problem you started with. Confirm patients can reply on the channel they choose and get a real answer back.
Ask how it handles HIPAA. A two-way thread carries symptoms, medications, and test results, so it needs the safeguards the HHS Office for Civil Rights expects: encryption, consent capture, access controls, and audit logging, with a business associate agreement in place. Get the specifics, not a compliance logo.
Ask how deep the EHR integration goes. Read-only isn't enough. Communication should write back to the record, or your care team ends up reconciling two systems by hand.
Ask where automation stops and people start. The platform should resolve routine volume on its own and escalate complex cases to staff, so you get the efficiency without dropping the patients who need a person.
These map to the broader questions health system leaders weigh when they build a digital front door, where communication sits alongside scheduling, intake, and care navigation.
Patient communication that patients respond to
Commure Engage brings these capabilities into one platform. It reaches patients across SMS, RCS, voice, and email, runs on 500+ clinically validated care pathways, and integrates bi-directionally with the EHR. More than 80% of patient inquiries resolve automatically, and outreach capacity scales up to 6.5x without adding staff.
What is patient communication software? Patient communication software is the platform a health system uses to reach and respond to patients across channels like text, voice, and email. Modern tools are two-way and AI-powered, so patients get answers and the care team stays in the loop, with everything connected to the EHR.
How is patient communication software different from an appointment reminder tool? A reminder tool sends one-way messages: appointment times, prep instructions, and alerts. Patient communication software adds a return path. Patients reply, get answers, and their responses route to the care team and into the EHR. The reminder becomes one feature inside a two-way system.
Is patient communication software the same as a patient portal? No. A portal waits for patients to log in. Patient communication software reaches patients on the channels they already use, like text and voice, and doesn't require a separate login or app.
Is texting patients HIPAA-compliant? It can be, with the right safeguards. Standard consumer texting isn't secure enough for protected health information. A HIPAA-compliant platform adds encryption, consent capture, access controls, and audit logging. The vendor also must sign a business associate agreement.
Who should own patient communication in a health system? It usually spans operations, IT, and clinical leadership, with input from marketing on voice and messaging standards. Operations owns the workflows, IT owns the EHR integration and security, and clinical teams shape the escalation and triage logic. Naming one accountable owner early keeps the program from fragmenting.
Hospitals lose about 3% to 5% of net revenue every year to revenue leakage, according to HFMA. Set that against the margin most systems actually operate on (the aggregate hospital operating margin is 5.2%), and the leak is roughly the size of the entire margin.
Most of that lost revenue gets chased after the fact. Retrospective chart audits, appeals on denied claims, quarterly reconciliation reviews. The work happens weeks or months after care was delivered, when the documentation has gone cold, and the filing window may already be closed.
Revenue integrity is the discipline built to stop that. It's the accuracy-and-compliance layer of the revenue cycle, and AI is moving it upstream: correctness enforced at the point of care, on every encounter, as it happens. That shift, from audit to assurance, is the story of this piece.
What is revenue integrity?
Revenue integrity is the practice of making sure what a health system documents, codes, and bills accurately reflects the care it actually delivered. The goal is to capture every dollar earned while staying compliant with payer and regulatory rules.
That means guarding accuracy in both directions. Under-capture costs you revenue you rightfully earned. Over-capture, like upcoding or billing for services that don't match the documentation, invites audits, recoupments, and compliance penalties.
In practice, healthcare revenue integrity spans several connected functions: clinical documentation, coding accuracy, charge capture, denial prevention, and underpayment recovery. A failure in any one of them surfaces downstream as lost or non-compliant revenue.
A revenue integrity function sits across clinical operations, coding, and billing, connecting teams that often work in silos. It ties the exam room to the balance sheet, which is where errors begin and where they get expensive.
Revenue integrity vs revenue cycle management
Revenue cycle management is the full pipeline: patient access, eligibility, charge capture, coding, claim submission, denials, and payment posting. It carries a service from delivery to payment.
Revenue integrity is the quality-control layer inside that pipeline. RCM asks whether a claim got paid. Revenue integrity asks whether it was right: coded to the correct level, supported by documentation, compliant, and complete.
You can run a fast revenue cycle that still leaks. Clean-looking claims get paid at the wrong amount, miss charges entirely, or trigger audits down the line. Revenue integrity is the check that keeps speed from turning into risk.
The documentation and coding accuracy pillar
Accurate reimbursement starts with accurate documentation. When a note fails to capture the full complexity of a visit, coders can't support the correct billing level, and the claim comes in low or wrong. The same gap distorts quality and risk-adjustment scores, since the codes that drive reimbursement also feed severity and outcomes reporting.
A service delivered but never charged never becomes a denial. It just disappears. That makes charge integrity the quietest form of revenue leakage and one of the hardest to catch.
Charges leak through lag, chargemaster mismatches, and manual processes that depend on someone remembering to enter a code. HFMA estimates as much as 1% of net charges are lost to charge integrity leakage, and its benchmarks call for capturing charges within 3 to 5 days and holding late charges under 2% of the total.
Denials are the visible symptom of upstream integrity failures. A denied claim usually points back to a documentation gap, a coding error, or an eligibility miss that happened well before the claim went out.
Commure customers using denial management tools with a pre-bill approach have cut pre-bill denials by 16% and reduced error rates by 35%, catching problems before claims are ever submitted.
How AI moves revenue integrity from audit to assurance
The traditional model is retrospective by design. Coders and revenue integrity teams review charts after discharge, auditors sample claims after payment, and appeals teams fight denials after the money's already been withheld. Each step catches some errors and misses others, and all of them cost time and staff.
AI changes the timing of that check, moving it to the moment care is delivered. During the visit, Ambient AI captures complete documentation while Autonomous Coding assigns accurate codes within seconds, each with its supporting rationale attached. On every encounter, Charge Note Reconciliation surfaces services that were documented but never billed, and denial tooling flags at-risk claims before they reach the payer.
Brought together on one platform, these steps make integrity continuous. Correctness gets built in as care is documented and coded, so fewer errors reach the claim and far fewer surface months later as denials or audit findings. It also means problems get caught while there's still time to fix them, before a filing window closes or a wrong claim goes out.
What a modern revenue integrity program looks like
A strong program is cross-functional by design, with clinical operations, coding, and billing sharing data and accountability across departments. It monitors continuously, flagging issues as they happen rather than collecting them for a quarterly cleanup.
Track the KPIs that expose leakage early: net collection rate (95% to 99% is the target), denial rate, charge lag, and avoidable write-offs held to 2% to 5% of net patient revenue, per HFMA. These numbers tell you where people, process, or technology are underperforming.
The technology layer, often called revenue integrity software, is what makes continuous checking practical at scale. The programs that get results treat revenue integrity as a revenue system in its own right, with the staffing, data, and executive attention that implies.
The bottom line
Revenue leakage runs about the size of a typical hospital's operating margin, and most of it still gets chased retrospectively. Revenue integrity closes that gap by keeping documentation, coding, and charges accurate from the start.
The move from audit to assurance is the real opportunity. AI makes correctness continuous, built into every encounter, so revenue integrity protects revenue in real time.
See how Commure RCM turns revenue integrity into a continuous process, from the exam room to the balance sheet.
Revenue leakage happens when care delivered doesn't fully convert into accurate, paid claims. The most common causes are incomplete clinical documentation, coding errors, missed or late charges, chargemaster mismatches, eligibility and authorization gaps, and denials that never get worked. HFMA estimates hospitals lose about 3% to 5% of net revenue to leakage each year, much of it invisible until a retrospective audit catches it.
What are revenue integrity KPIs?
Revenue integrity KPIs are the metrics that show where accuracy breaks down and revenue slips away. The core set includes net collection rate (95% to 99% is the target), initial and final denial rates, clean claim rate, first-pass rate, charge lag (capture within 3 to 5 days), late charges (under 2% of the total), and avoidable write-offs (held to 2% to 5% of net patient revenue). Tracking them continuously, rather than reviewing them quarterly, is what lets teams catch problems while there's still time to fix them.
Why is revenue integrity important in healthcare?
Revenue integrity matters because the money at risk is roughly the size of a hospital's entire operating margin. Hospitals lose an estimated 3% to 5% of net revenue to leakage each year, while aggregate operating margins run around 5.2% and close to 4 in 10 hospitals operate in the red. Getting documentation, coding, and charges right protects the revenue a health system earned and keeps it compliant, which guards against both lost income and payer audits.











.jpg)