





A new patient in one of the 15 largest metro areas in the U.S. now waits an average of 31 days to see a physician, according to AMN Healthcare's 2025 survey, and rural patients often wait longer still (roughly 20% of Americans live in rural areas while only about 9% of physicians practice there, according to the National Rural Health Association). That wait is a symptom of a system that loses patients before the patient journey ever begins, and every day of delay is a chance for someone to switch providers, defer care, or disappear from the schedule entirely.
The patient journey is the full arc of a person's experience with a health system, from the first symptom or online search, through treatment and long-term follow-up. Health systems have mapped that journey for years, yet far fewer have fixed the gaps along the way.
This guide covers what the patient journey is, the stages every patient moves through, how to map it, and how to close the gaps that quietly cost health systems patients and revenue.
What is the patient journey?
The patient journey is the sequence of interactions a person has with a healthcare organization over time, starting well before a first appointment and continuing long after a visit ends. It covers how someone finds a provider, books and prepares for care, moves through the visit itself, and stays connected for follow-up and ongoing needs.
Much of the healthcare patient journey plays out beyond the exam room: the phone tree at scheduling, the intake form, the reminder that does or doesn't arrive, the call after a procedure when a question comes up at 9 p.m.
It helps to separate two terms that often get used interchangeably. The patient journey is what actually happens to the patient. A patient journey map is the tool you build to see that experience clearly and decide what to change.
Why the patient journey matters
Healthcare has shifted from a system patients accepted to one they shop, and people now compare providers the way they compare any other service. That shift shows up plainly in switching behavior. About 1 in 5 patients switched providers in the past year, and nearly 90% of them did so because the organization was hard to do business with, according to an Accenture survey reported by the American Hospital Association. 7 in 10 pointed to access as a deciding factor when they chose someone new.
That pattern points squarely at the friction around care: the busy phone line, the confusing bill, the message that never gets a reply. Every one of those friction points sits somewhere on the patient journey, which is why mapping it and fixing what you find has become a retention strategy in its own right.
The stages of the patient journey
Most patient journeys move through 6 stages: awareness, consideration, access, the visit, follow-up, and ongoing care. Few patients travel them in a tidy line, since people loop back, pause, or drop out along the way, but the stages give you a shared structure for pinpointing where the experience breaks down.
Awareness
Awareness starts the moment someone notices a symptom or decides they need care. Most people begin with a search engine rather than a physician referral, so the clarity of what they find shapes their first impression of your organization long before they ever call. Content that answers real questions, a findable location listing, and current reviews all work well at this stage.
Consideration
In the consideration stage, patients weigh their options against practical criteria: location, accepted insurance, reviews, and whether they can actually reach you. This is where many patients silently choose a competitor, often for reasons that have nothing to do with clinical quality. A booking page that asks for too much, a call that goes to voicemail, or a week-long callback delay can end the relationship before it begins.
Access
Access is where the journey stalls more often than not. With new-patient waits averaging a month across major metros, the organizations that win patients are the ones that make scheduling fast and answer the phone reliably.
Access is also one of the more fixable stages. One community health center that began handling inbound calls with AI call center agents saved 800 labor hours for every 10,000 calls, roughly $240,000 a year, while resolving a large share of requests without staff involvement. Widening patient access at the front door keeps patients from giving up before they arrive.
Preparation belongs to this stage too. Long paper forms and prep instructions that are easy to miss create no-shows and day-of delays, which is why modern patient intake moves the clipboard onto the patient's phone through conversational outreach. Timely, multi-touch reminders that patients can actually respond to help reduce no-shows and protect both the schedule and the revenue attached to it.
The visit
The visit is where clinical care happens and where traditional patient-satisfaction measurement concentrates, spanning check-in, the encounter, and discharge. It's also where communication gaps take root, since patients often leave without asking the questions that mattered most to them and forget a large share of what they were told once they get home. What happens over the following days depends heavily on how well the visit sets them up.
Follow-up
Follow-up is the stage health systems most often let slide, even though it's where good clinical work can come undone. A 2026 study of more than 579,000 Medicare admissions found that many high-risk patients never receive post-discharge follow-up, and those who did were significantly less likely to be readmitted within 30 days. After a procedure, patients navigate medication questions, recovery uncertainty, and handoffs between care teams, and every handoff is a point where someone can slip through the cracks.
Two strategies make a measurable difference here. Tighter transitions of care keep information from getting dropped as a patient moves between settings, and proactive outreach closes the post-surgical care gap during the window when patients are home and most likely to need answers.
Ongoing care
Ongoing care turns a single visit into a lasting relationship that supports better health. For someone managing a chronic condition, this stage can stretch across years, and it's where loyalty is either earned or lost. Steady, personalized chronic care management keeps patients engaged between appointments, surfaces problems earlier, and reduces the avoidable complications that pull people back into acute care.
Patient journey mapping
Patient journey mapping is the practice of laying out each stage, touchpoint, and emotion a patient experiences, so you can see where the journey serves them and where it fails them. The patient journey map is the visual result, a shared picture of what patients do, think, and feel as they move through your system.
Here is a very basic example of a patient journey map. The more details you can fill in, the better.
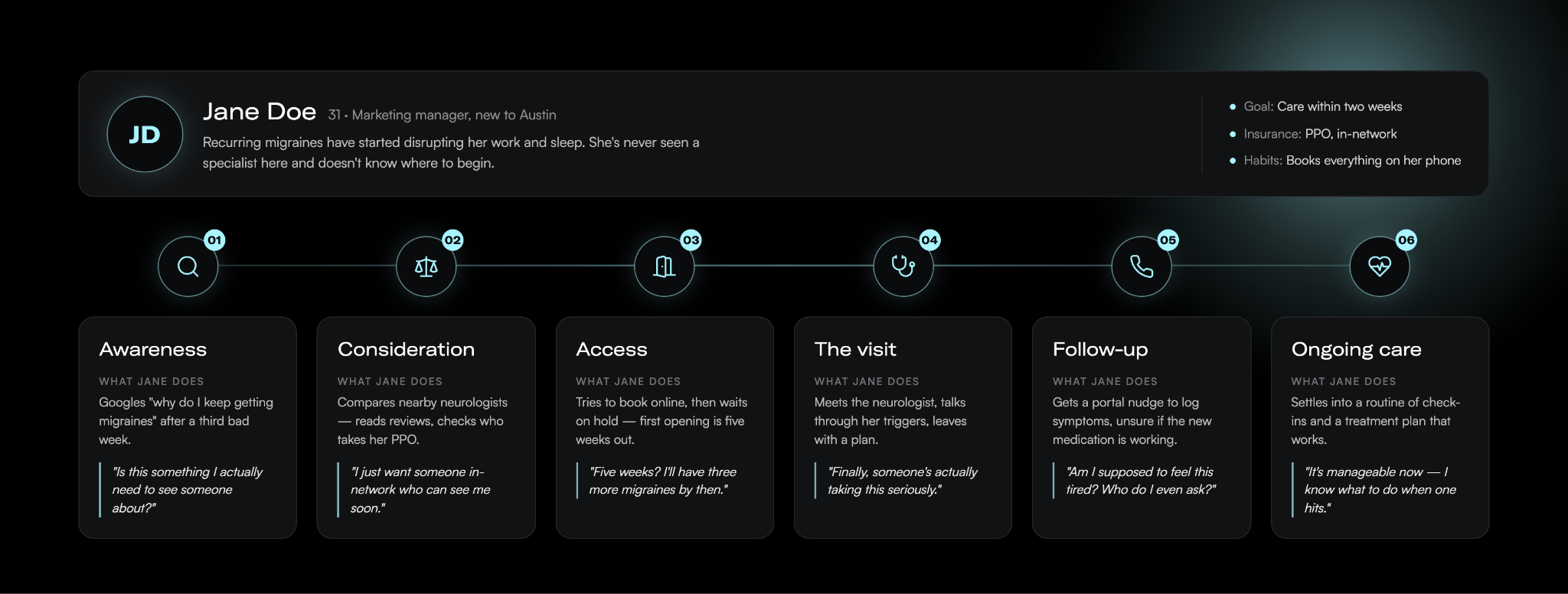
Done well, a map earns its keep in a few ways. It creates a common view of the experience across departments that rarely talk to each other, exposes the specific moments where patients get stuck, and turns vague complaints about "patient experience" into a prioritized list of fixable problems.
Types of patient journey maps
Teams generally build one of four map types depending on the question they're answering.
A current-state map shows the journey as it runs today, drawn from real patient data, and it's the right starting point for incremental improvement.
A future-state map describes the journey you want to deliver and works well for aligning teams around a new service or process.
A day-in-the-life map widens the lens to what a patient experiences outside your system, which helps you spot unmet needs you'd otherwise miss.
A service blueprint goes the other direction and adds the people, systems, and policies behind each touchpoint, so you can trace a pain point back to the process that caused it.
Most organizations start with one type and add others as the work matures.
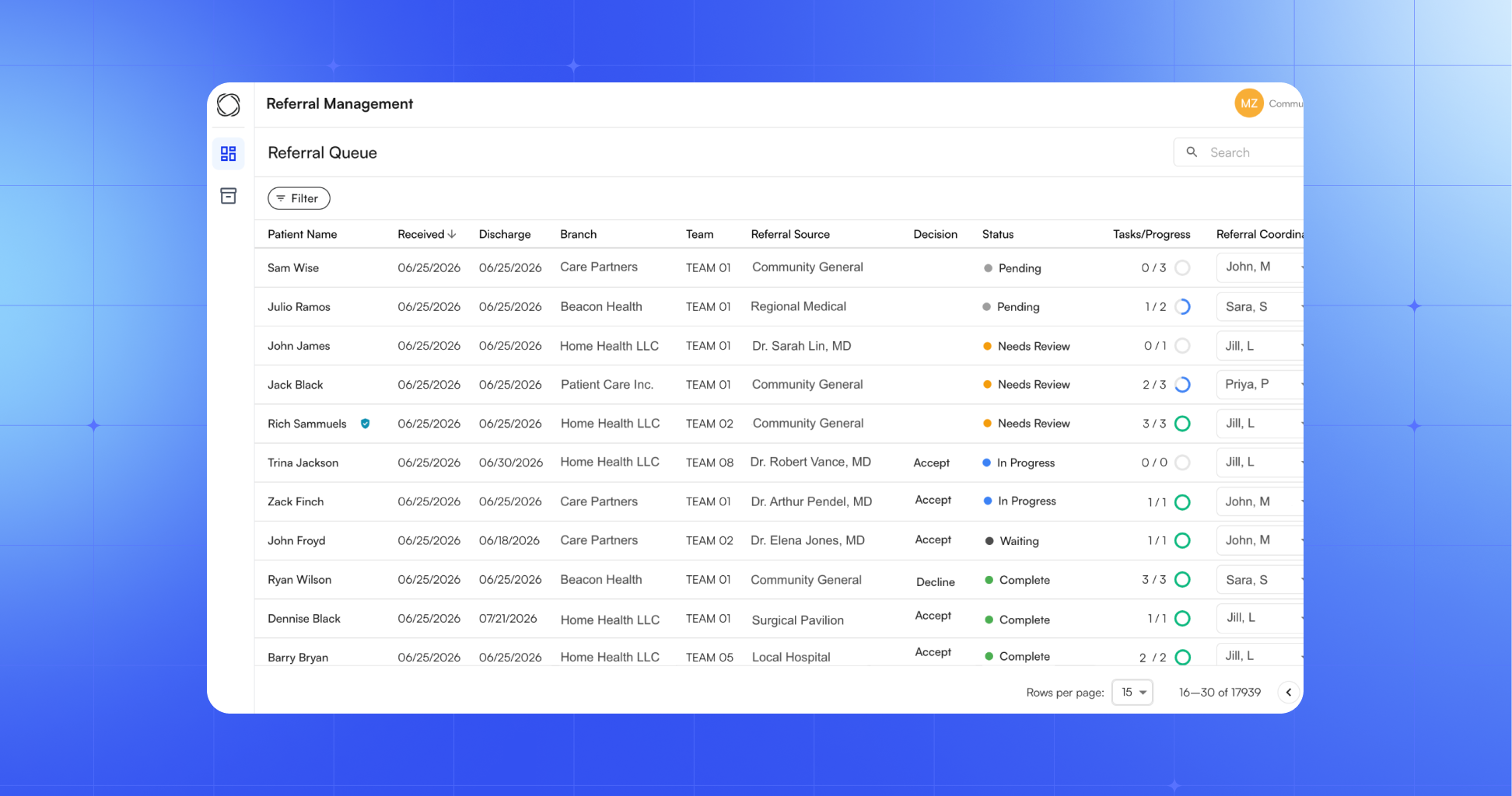
Patient journey analytics
The strongest maps sit on data. Patient journey analytics is the practice of layering your operational and experience data onto the map: scheduling and no-show records, call-center hold times, message response rates, portal usage, and post-visit feedback. Those numbers show you where patients actually drop off rather than where you assume they do, and they let you measure whether a change at one touchpoint moved the outcome you cared about.
How to map the patient journey
Here are the steps to take to build out your patient journey map:
- Define your scope and goal. A map can zoom in on a single interaction, like booking an appointment, or span an entire condition, like managing diabetes over several years. Let the problem you're trying to solve set the boundaries.
- Gather data from multiple sources. Combine direct patient input from interviews, surveys, and short diary studies with the operational and experience data you already hold, like scheduling records, message response rates, and existing patient satisfaction and engagement survey scores. Interviews add depth, surveys validate patterns at scale, and the data you already collect grounds the whole map in what really happens.
- Build personas. A new mother's journey looks nothing like an oncology patient's, so segment by the populations you actually serve rather than mapping a generic average patient.
- Chart touchpoints and emotions. For each stage, record what the patient does, who and what they interact with, and how they feel. The emotional low points usually mark your biggest opportunities, since that's where frustration leads to a decision to leave.
- Validate and act. Put the draft in front of patients and frontline staff to catch what you missed, then commit to fixing the touchpoints it exposes. A map only pays off when it drives real changes to how you operate.
Common mapping mistakes
A few mistakes hurt the value of patient journey mapping. The most common is treating the finished map as the deliverable, when the map only matters once it changes how you work. Others include mapping the journey your organization wishes patients took instead of the one they actually take, building the whole thing from internal assumptions without talking to a single patient, and mapping so broadly that no team owns any specific fix. Assigning clear ownership for each stage, and revisiting the map as your services and patients change, keeps it from going stale.
Closing the gaps
Finding the gaps is the easy part; closing them, stage by stage, is where patient experience actually improves and where retention follows.
In practice, that means answering the phone during the access stage, replacing paper intake with conversational outreach before the visit, and staying in contact through follow-up and ongoing care instead of going quiet once the encounter ends. The connected set of tools that supports patients across all of these stages is what many health system leaders now call the digital front door, and it works best as a single platform that writes back to the EHR rather than a stack of disconnected point solutions. Keeping patients informed between visits is the job of patient communication software that reads each reply and routes anything a human needs to handle to the right person.
Commure Engage is built for exactly this work, supporting front-cycle patient experience across scheduling, intake, communication, and care navigation on one platform. Yale New Haven Health used Commure Engage for pre-appointment outreach in its breast imaging program and cut no-show and same-day cancellation rates by more than half.
Map the journey your patients actually take, then close the gaps one stage at a time. See how it all comes together.
Frequently asked questions
What is the difference between the patient journey and the patient experience?
The patient journey is the full sequence of steps a patient moves through, from first symptom to ongoing care. The patient experience is how they perceive and feel about those steps. The journey is the path, and the experience is the quality of each interaction along it, which is why you map the journey to improve the experience.
What are the stages of the patient journey?
The patient journey typically moves through 6 stages: awareness, when someone notices a symptom; consideration, when they weigh providers; access, when they schedule and prepare; the visit, when care happens; follow-up, after a procedure or discharge; and ongoing care, which sustains the relationship over time. Few patients travel them in a straight line.
Who is responsible for the patient journey in a health system?
No single department owns the patient journey, which is part of what makes it hard to fix. It crosses scheduling, front-desk staff, clinicians, billing, marketing, and IT, so improving it takes shared ownership rather than one team's effort. Most organizations assign an owner for each stage plus a cross-functional group to keep the full journey aligned.
How can health systems improve the patient journey?
Health systems improve the patient journey by fixing the touchpoints a journey map exposes, stage by stage. The biggest gains usually come at access: answering the phone, offering online self-scheduling, and replacing paper intake with digital outreach. A July 2025 MGMA poll found 71% of practices have less than 25% of their patients using digital tools to self-schedule, so the opportunity is wide open.



.jpg)



.jpg)
.jpg)
