







In healthcare, what gets documented gets paid for. What doesn't, doesn't.
That simple equation is why clinical documentation improvement (CDI, also known as clinical documentation integrity) has become one of the most consequential disciplines inside modern health systems. CDI sits at the intersection of clinical care, coding accuracy, regulatory compliance, and revenue. When it works, hospitals get paid appropriately for the care they deliver. Quality scores reflect reality. Clinicians spend less time chasing queries.
When it doesn't, the costs compound, resulting in denied claims, underpayments, distorted quality metrics, and frustrated providers.
The discipline isn't new. But the way leading health systems approach it is changing fast. The traditional CDI playbook was built around manual chart reviews and retrospective physician queries, designed for an era of paper records and fee-for-service billing. AI is rewriting that playbook.
Here's what CDI is, why it matters more than ever, and how AI is changing the way health systems approach documentation.
What is clinical documentation improvement?
Clinical documentation improvement is the practice of making sure a patient's medical record accurately reflects their clinical condition, the care they received, and the medical decision-making behind it. Done well, CDI bridges the gap between clinical reality and what eventually shows up on a claim form.
A traditional CDI program runs on certified specialists, usually nurses or coders with additional credentials. They review patient charts, identify gaps or ambiguities, and submit queries to physicians for clarification. They work alongside medical coders to make sure diagnoses are documented with the specificity required for accurate ICD-10 and CPT coding, that complications and comorbidities (CCs and MCCs) are captured, and that the final claim reflects the true acuity of the patient.
AHIMA's guidance for CDI programs frames the discipline as foundational to accurate reporting under CMS quality measures, value-based purchasing, and DRG-based payment.
Documentation determines whether a chart reflects the full acuity of a patient, and that distinction often drives thousands of dollars per case in reimbursement. A patient documented with a major complication or comorbidity (MCC) can generate more than double the payment of an otherwise identical chart without one. The clinical reality is the same. The documentation is what changes the number.
A peer-reviewed study in the Journal of Vascular Surgery found that a physician-led CDI initiative significantly increased the case mix index and contribution margin. That finding has been replicated across specialties and care settings.
This is also why CDI is foundational to revenue cycle management. Coding, claim submission, denials prevention, reimbursement: they all depend on documentation that meets payer and regulatory standards, with CDI sitting upstream of all of it.
Why clinical documentation improvement matters
CDI isn't a back-office function. Its impact shows up in three places every health system executive cares about: revenue, quality, and clinician experience.
Financial impact. Strong CDI programs have a direct line to the bottom line. AHIMA's Clinical Documentation Improvement Toolkit identifies CDI as one of the most effective levers a hospital has for reducing denials, capturing severity of illness and risk of mortality, and securing appropriate reimbursement. Health systems using modern CDI tooling embedded in EHR workflows have seen revenue gains of up to 3% when documentation gaps are flagged in real time. For an enterprise health system, 3 points of net patient revenue could be the difference between hitting and missing a year.
Clinical quality and risk adjustment. Documentation determines how the outside world sees a hospital's quality. Mortality indices, publicly reported outcomes, case mix index (CMI), and risk-adjusted payment under value-based contracts all flow from what gets documented. CMS continues to expand value-based care arrangements, which makes precise documentation a revenue, quality, and contractual question all at once.
Regulatory complexity. The documentation bar keeps rising. The WHO's ICD-11 update introduced roughly 17,000 new diagnostic categories, and the 2025 Medicare Physician Fee Schedule ties more of reimbursement to documentation precision. The global CDI market is projected to grow from $4.88 billion in 2024 to $10.44 billion by 2034, a clear signal that health systems recognize the cost of getting documentation wrong.
The pressure is increasing right when CDI capacity is shrinking. Two-thirds of HIM leaders cite staffing shortfalls that directly impact revenue integrity, and the workforce of qualified CDI specialists isn't expanding fast enough to close the gap.
The problem with the traditional CDI model
The old CDI playbook is running out of road for one fundamental reason. It relies on humans reviewing charts after the fact, and there aren't enough humans to do it.
Clinicians are already drowning in documentation. Research from Annals of Family Medicine and cited by the AMA shows that physicians spend 5.9 hours of an 11.4-hour workday in the EHR. An AJMC analysis found 76.1% of office-based physicians spend more than an hour per day documenting outside clinic hours, averaging nearly 2 hours of "pajama time" daily. The AMA identifies clinical documentation as one of the leading contributors to physician burnout.
Layering more retrospective queries onto already-burned-out physicians is a tax. And it's a tax that traditional CDI programs depend on to function.
How AI is reshaping clinical documentation improvement
The real shift in CDI isn't faster query workflows or better dashboards. It's that AI moves documentation improvement from a retrospective discipline to a real-time one.
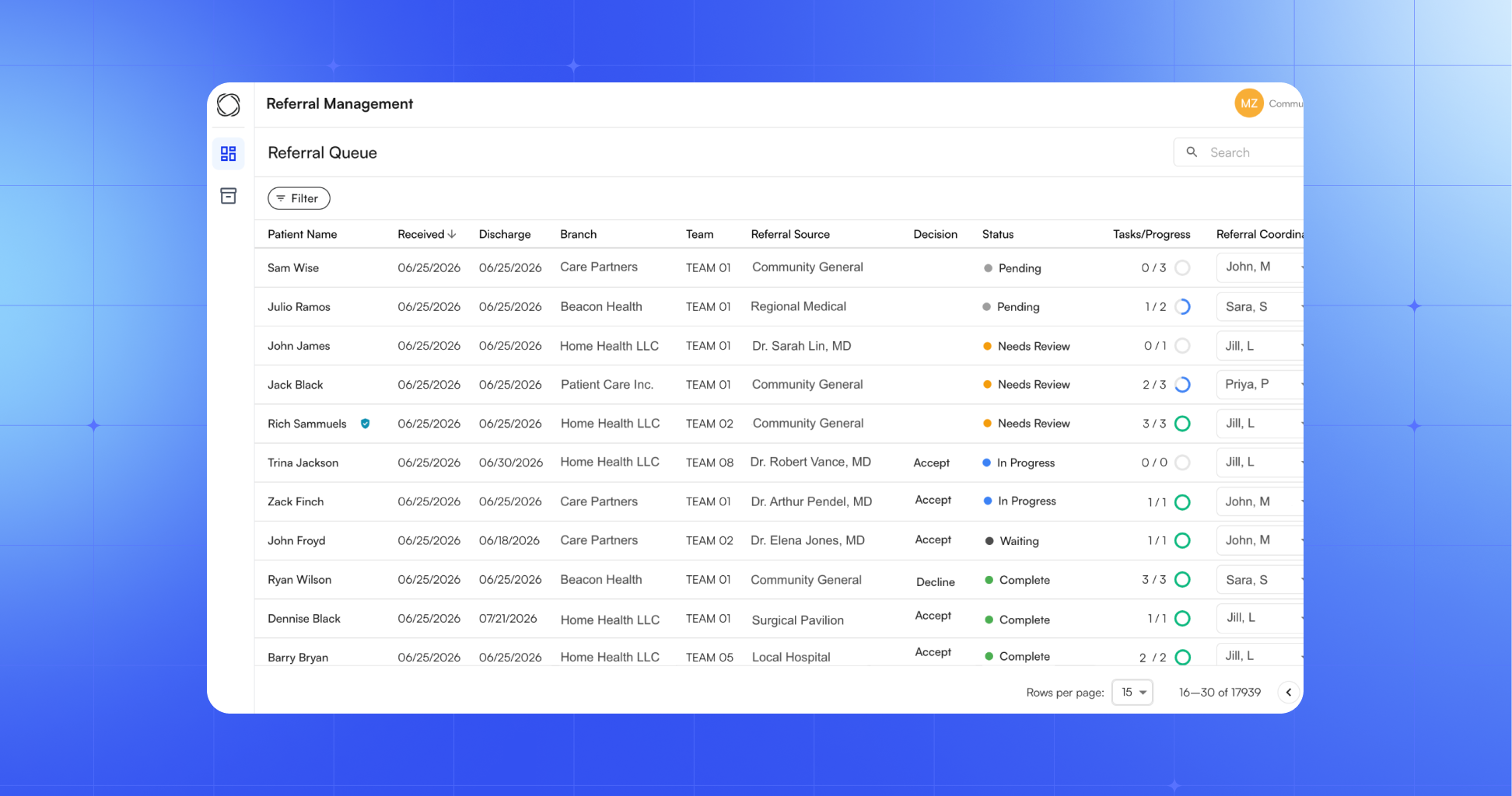
Ambient AI captures the clinical picture as it happens. A clinician used to dictate a stripped-down note after the visit, then a CDI specialist would query for missing details days later. With ambient AI listening to the encounter, structuring the note in real time, and surfacing CareCues during the visit itself, the documentation gap closes before it opens.
AI-assisted CDI expands specialist capacity. According to MedLearn Publishing's analysis of AI in clinical documentation integrity, CDI specialists augmented by intelligent systems can manage 35–45% larger chart volumes, which lets organizations expand CDI coverage without proportional staffing increases. The same analysis reports 12–18% denial reductions for complex inpatient stays and 20–25% reductions on prior authorization submissions when AI-assisted CDI is deployed at scale.
Autonomous coding closes the loop from documentation to claim. When documentation is captured cleanly in real time, AI can generate accurate CPT codes, ICD-10 diagnoses, and modifiers directly from the clinical note. In a deployment with Ob Hospitalist Group, Commure's Autonomous Coding generated 85% of CPT and ICD-10 codes and reduced charge entry time by 83%. At a leading NYC health system, the combination of ambient documentation, charge note reconciliation, and autonomous coding drove a 20% increase in monthly charges and cut late-filing denials in half.
These gains reflect a different operating model for CDI, one where documentation improvement is built into the workflow itself instead of bolted on afterward.
What to look for in a modern CDI approach
For health system leaders evaluating where CDI is headed, four questions matter:
- Is documentation improved in real time or retrospectively? Real-time intervention prevents errors. Retrospective intervention chases them.
- Is the system EHR-integrated or bolted on? CDI that requires clinicians to switch contexts or duplicate work won't get adopted.
- Does it connect documentation to coding to claims? The biggest gains come from treating the documentation-to-reimbursement pipeline as one continuous workflow instead of three disconnected ones.
- Is it built for enterprise scale? Pilots are easy. Sustained CDI improvement across hundreds of providers and dozens of specialties is the real test.
The health systems pulling ahead on documentation today are rebuilding CDI around AI that works at the point of care and connects clinical documentation directly to the revenue cycle


.jpg)



.jpg)
.jpg)
