




ChatGPT for Doctors: How to Use AI in Your Practice in 2026
A practical guide to using ChatGPT and purpose-built clinical AI tools in solo and group practices, with a clear breakdown of what each tool actually does.
Written by the Commure Scribe Team
Published: April 10, 2026
•
9 min read
Updated June 30, 2026
What You Need to Know About ChatGPT for Doctors
- Physicians use ChatGPT and other AI tools to draft notes, write prior auth letters, create patient education materials, and cut admin time.
- General ChatGPT is not HIPAA-compliant and does not capture live visits. Purpose-built clinical AI tools handle those gaps.
- This guide covers what each tool does and where each fits.
Physicians across solo and group practices have been experimenting with ChatGPT for doctors since late 2022. The use cases were immediate and practical: prior auth letters drafted at midnight, patient-friendly discharge summaries, differential lists on tough cases. ChatGPT cut time on those tasks.
The landscape has grown since then. General-purpose ChatGPT is one option. Clinical AI tools built specifically for medicine are another. Each solves a different problem. This guide covers how to use ChatGPT for doctors, where it falls short, and what purpose-built tools handle that general AI cannot.
What Is ChatGPT, and How Are Doctors Using It?
ChatGPT is a large language model (LLM) built by OpenAI. It generates text from patterns learned in a large training corpus. Give it a prompt and it produces a response based on those patterns.
Doctors use it as a writing and reasoning assistant. It does not connect to your EHR, does not listen to visits, and does not have access to your patient's records. Its value is in generating well-structured text from inputs you provide.
"ChatGPT for doctors" has also become shorthand for a broader category of clinical AI. Three distinct tools now carry that label:
- General-purpose LLMs (ChatGPT, Claude, Gemini): writing tasks, summaries, admin work, de-identified drafting.
- Clinical decision support AI (OpenEvidence and similar): evidence lookups, differential support, guideline search. Trained on medical literature, not general web data.
- Ambient documentation AI: real-time visit capture, structured note generation, EHR integration.
Each solves a different job. Most of what physicians search for under "ChatGPT for doctors" falls into the first category. The rest of this guide focuses there.
The taxonomy matters because the search term "ChatGPT for doctors" now covers all three, and choosing the wrong tool for the job wastes time.
What Can Doctors Use ChatGPT For?
General-purpose LLMs handle tasks that are primarily linguistic. The physician does the clinical work. The AI handles the writing. In practice, those tasks include:
Note drafting. Paste a de-identified visit summary into ChatGPT and ask for a SOAP note. The output is often well-structured and cuts writing time. Review and edit before it enters the record. Hallucination rates make physician review essential.
Prior auth letters. AI handles the structure of a prior auth appeal well: clinical summary, medical necessity argument, supporting criteria. A 20-minute letter can be drafted in under 5 minutes. Review for accuracy before sending.
Patient education materials. ChatGPT handles plain-language explanations well: new diagnoses, post-procedure care, drug side effects. Paste a clinical summary and ask for a patient-facing version at an 8th-grade reading level. Review before use.
Differential brainstorming. Enter a clinical presentation and ask for a differential list. This surfaces diagnoses worth considering. It works as a checklist prompt, not a diagnostic engine.¹
CME prep and education. Residents and practicing clinicians use LLMs to generate practice questions, explain mechanisms, and summarize guidelines. Research in education contexts is generally positive.²
Admin writing. Referral letters, payer inquiry drafts, internal protocols, and staff memos all save time here. No clinical risk is involved.
These tasks share one trait: none capture a live patient visit. The physician does the clinical work. The AI helps with the writing afterward.
What Are the Limitations of ChatGPT in Clinical Practice?
The limitations of ChatGPT for doctors fall into five categories.
Hallucination. LLMs produce text that sounds right but is sometimes factually wrong. A 2023 PMC study found ChatGPT fabricates citations and misquotes drug dosages.³ It also makes confident errors in clinical reasoning tasks. Physician review catches these errors. No current LLM has solved this problem.
Outdated knowledge. ChatGPT has a training cutoff. Guidelines change. Drug recalls happen. The model has no knowledge of evidence published after its training date. Verify outputs against live sources for current treatment standards.
No patient context. ChatGPT has no access to patient history, problem lists, or medications. It cannot pull from your EHR. Paste that data into the prompt, or the model works blind. This limits its value to text generation tasks only.
Weak performance on complex cases. ChatGPT handles board-style questions well. Complex cases with conflicting findings or judgment under uncertainty expose its limits.⁴ Simple presentations get more reliable suggestions than complex ones. Decision support is most valuable exactly where performance is weakest.
No learning across sessions. ChatGPT does not adapt from corrections. Fix an incorrect note structure in the prompt. It will not carry that fix to the next session.
Is ChatGPT HIPAA-Compliant for Clinical Use?
This is the question most small practices get wrong about ChatGPT for doctors.
No, standard ChatGPT is not HIPAA-compliant for clinical use.
Standard ChatGPT does not include a Business Associate Agreement (BAA). HIPAA needs any vendor handling protected health information (PHI) for a covered entity to sign a BAA. If you enter patient identifiers, dates of service, or diagnoses into a standard ChatGPT session, that creates a HIPAA risk.
OpenAI now offers three healthcare-specific tiers. ChatGPT for Clinicians launched on April 22, 2026, and is free for any verified U.S. physician, nurse practitioner, physician assistant, or pharmacist. It includes optional HIPAA support through a Business Associate Agreement.
ChatGPT for Healthcare is the enterprise tier, built for enterprise-wide institutional deployment with HIPAA compliance, customer-managed encryption keys, and BAAs. Standard consumer ChatGPT remains outside this compliance framework. If you are a verified U.S. clinician, ChatGPT for Clinicians is the free on-ramp with HIPAA cover available. Enterprise deployments go through ChatGPT for Healthcare.⁵
Three categories of ChatGPT use by compliance risk:
- No PHI tasks: Admin writing, staff training materials, guideline summaries, patient education templates with no patient-specific data. No HIPAA exposure. ChatGPT works here without compliance concerns.
- De-identified inputs: Note structures drafted from a clinical scenario stripped of all 18 HIPAA identifiers. Compliant, but needs a consistent de-identification process and reduces utility because the AI lacks patient context.
- PHI tasks: Any task where patient-specific data enters the prompt. Needs a HIPAA-compliant platform with a signed BAA. Standard consumer ChatGPT is not that platform.
Practices that want AI inside their clinical workflow with real patient context need a purpose-built tool. ChatGPT for doctors in its standard form does not provide that.
How Does ChatGPT Compare to Clinical AI Tools Built for Doctors?
The ChatGPT for doctors landscape now spans three distinct tool categories. General ChatGPT is a generalist. Purpose-built clinical AI tools train on medical data, integrate with clinical workflows, and carry compliance infrastructure by design.
Three categories now compete for the "ChatGPT for doctors" label:
General-purpose LLMs (ChatGPT, Claude, Gemini). Best for de-identified writing tasks: note drafting from summaries, prior auth letters, patient education, admin writing. No HIPAA cover by default. No real-time visit capture. No EHR connection.
Clinical decision support AI (OpenEvidence and similar). OpenEvidence is the tool most media outlets call "ChatGPT for doctors." It trains exclusively on peer-reviewed journals and guidelines, cites every claim, and withholds answers when uncertain. It has a large and growing base of verified physician users.⁶ It handles evidence lookups, differential support, and guideline search. It does not generate visit notes or touch documentation workflow. Free for individual clinicians.
Ambient documentation AI. These tools listen to a live physician-patient conversation and produce a structured clinical note from the audio. The clinician does not type, paste, or prompt. HIPAA-compliant by design. EHR integration built in. These tools solve the documentation burden clinicians face today.
The practical split: use general ChatGPT for de-identified writing tasks. Use OpenEvidence for clinical questions. Use an ambient documentation tool for notes.
What Is Ambient Documentation AI, and How Does It Differ from ChatGPT?
Ambient tools listen to a physician-patient conversation and produce a clinical note from the audio. The clinician does not type, paste, or prompt. The tool captures the visit as it happens.
This is where ChatGPT for doctors in its standard form stops and purpose-built ambient AI begins.
Ambient scribes use LLMs as a core component. The surrounding setup is not the same as ChatGPT:
- Real-time capture. The tool listens during the visit and processes audio through medical language models. The note comes from the conversation, not from a post-visit summary.
- EHR connection. Clinical-grade tools connect directly to EHR systems. Notes land in the record without copy-paste. Enterprise tiers use bidirectional API sync. Copy-paste is available at lower tiers.
- HIPAA by design. Ambient scribe platforms include BAAs, compliant data storage, and documented audio retention policies. Audio handling varies by vendor. Confirm the policy before you sign.
- Structured output. Notes come out as SOAP, DAP, or specialty templates. The tool suggests ICD-10 and CPT codes. The clinician reviews and approves. Review time per note is brief.
The workflow difference:
General ChatGPT: see patient, write notes or dictate, paste de-identified summary, prompt LLM, paste output into EHR, edit.
Ambient scribe: see patient (tool runs in background), click End Recording, review and approve the note in the EHR.
The clinician stays present in the room. Note-taking runs in the background.
What Does Research Say About AI Documentation Tools in Practice?
Research on ChatGPT for doctors and AI documentation tools has grown since 2023, but results are not uniform.
A 63-week study from the Permanente Medical Group covered 7,260 physicians and 2.5 million encounters. It found charting time savings of 15,791 hours across the cohort. High users saved 2.5 times more time per note than low users. Physician age showed no link to adoption rates.⁷
A 2025 UCLA randomized trial of 238 physicians across 14 specialties found that one of two AI scribes tested—Nabla—reduced note-writing time by 9.5% compared to usual care; the other tool showed no statistically significant change. Both tools showed modest improvements in burnout and cognitive workload scores.⁸ A separate analysis of primary care physicians at Massachusetts General Hospital and Brigham and Women's Hospital found they spent an average of 36.2 minutes on EHR tasks per 30-minute scheduled visit, including 6.2 minutes of after-hours "pajama time" per visit.⁹ After-hours EHR time has gotten worse year over year. Headline burnout rates have slightly improved in that period, but the documentation burden has not.
Not all studies are positive. A Cleveland Clinic study of high-burden primary care physicians found one significant change from AI scribe use: fewer characters typed. Same-day chart closure fell 3%. After-hours work increased, though not significantly. Mean likelihood to recommend scored 6.5 out of 10.¹⁰
Note bloat is also documented. Some physicians produce longer notes with AI. The tool captures detail that manual notes skip. Longer notes are not better notes. Payers have flagged upcoding concerns in some cases.
The evidence is strong in direction but mostly comes from large health systems. Those systems carry IT support most practices do not have. Run your own trial on your own visit volume. Do not project system-level numbers onto your clinical setting.
What Should Doctors Look for When Evaluating Clinical AI?
Practices evaluating ChatGPT for doctors and purpose-built clinical AI tools hit the same decision points. Work through these first:
- BAA availability. Confirm a BAA is included at the tier you are buying.
- Audio handling. Audio from a patient visit is PHI. Ask how the tool stores, encrypts, and retains recordings. Policies vary significantly across vendors. Get the specifics in writing.
- EHR connection. Copy-paste works at all practice sizes. API sync is available from most vendors at enterprise tiers. On Athenahealth, eClinicalWorks, or similar named EHR systems, confirm named integration support. Do not rely on "works with most EHRs" language.
- Specialty support. Note templates vary by specialty. Confirm the tool has templates for your visit type or offers customization options.
- Review step. Confirm there is an approval step before the note is finalized. No tool should push notes to the chart without clinician review.
- Evaluation period. Some tools offer an ongoing free tier with volume limits. Others offer a 7-day expiring trial. A 7-day trial gives you enough visits to judge note quality for your specialty.
Commure Scribe: How It Works for Solo and Group Practices
Where ChatGPT for doctors falls short on live visit capture and HIPAA-compliant documentation, ambient scribes are built to fill that gap.
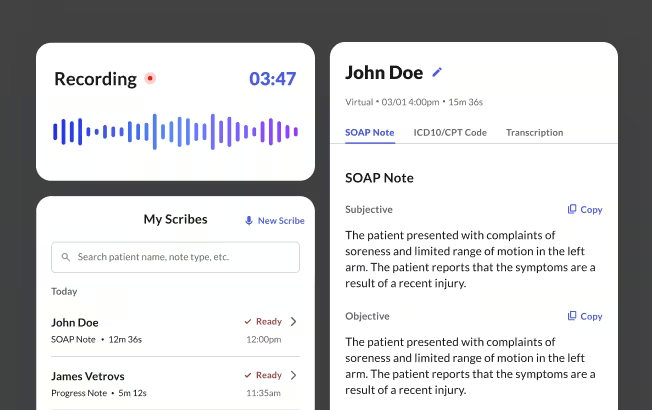
Commure Scribe captures the physician-patient conversation and produces a structured SOAP note in seconds. Click Start Recording at the top of the visit, see the patient, click End Recording. The note appears with suggested ICD-10 and CPT codes. Review, edit if needed, and finalize — via copy-paste or one-click EHR sync. Audio is encrypted and retained per HIPAA requirements. A BAA is included at all tiers.
It integrates with 60+ EHRs, including AdvancedMD, Elation Health, eClinicalWorks, athenahealth, and Tebra. Supports 90 languages with automatic detection. Works across internal medicine, family medicine, pediatrics, and more. Templates are customizable by specialty.
Frequently Asked Questions
Yes, with caveats. ChatGPT drafts notes from de-identified summaries. It does not capture live visits and does not connect to your EHR. Keep patient-specific data out of a standard ChatGPT session. No BAA means no compliance cover. Ambient tools handle this by design.
The main risks are hallucination, outdated knowledge, no patient context, and HIPAA compliance gaps. Physician review before content enters the record is the primary safeguard. Purpose-built clinical tools address specific risks: OpenEvidence reduces hallucination for clinical questions, ambient scribes handle HIPAA-compliant documentation.
Three categories cover the landscape. Clinical decision support: OpenEvidence (free for individual clinicians). Ambient documentation: Commure Scribe, Freed AI, Nabla, Heidi Health, Suki, DAX Copilot, Abridge, DeepScribe. General-purpose LLMs: ChatGPT, Claude, Gemini for de-identified writing tasks. Each category solves a different problem.
OpenEvidence is a clinical decision support tool trained on peer-reviewed journals and guidelines. Major media outlets use "ChatGPT for doctors" to describe it. It handles evidence lookups, differential support, and guideline search.
Standard consumer and Plus ChatGPT does not include a BAA. ChatGPT Enterprise offers a BAA for qualifying contracts. No BAA means entering PHI creates HIPAA exposure. Use a tool with a BAA built in for any PHI workflow.
Set the review requirement first: the clinician always has the choice to review the note before it goes to the chart. Run a trial across at least two to three weeks and multiple visit types. Pick one workflow owner to set up templates and answer questions from other providers. Use the onboarding support most vendors include. Medium and larger practices should set a brief written policy on AI use in charting before rollout.
Sources
- JMIR Medical Education. (2023, December 21). Using ChatGPT for Clinical Practice and Medical Education: Cross-Sectional Study. https://mededu.jmir.org/2023/1/e50658/
- ScienceDirect. Using ChatGPT for Clinical Practice and Medical Education. https://www.sciencedirect.com/org/science/article/pii/S2369376223000880
- National Center for Biotechnology Information. (2023, June 27). Utility of ChatGPT in Clinical Practice. PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC10365580/
- Topaz, M., Peltonen, L.M. & Zhang, Z. Beyond human ears: navigating the uncharted risks of AI scribes in clinical practice. npj Digit. Med. 8, 569 (2025). https://doi.org/10.1038/s41746-025-01895-6
- OpenAI. ChatGPT Enterprise. https://openai.com/enterprise
- HLTH. (2026, January 21). OpenEvidence Doubles Valuation to $12bn as Physician Adoption Accelerates. https://hlth.com/insights/news/openevidence-doubles-valuation-to-12bn-as-physician-adoption-accelerates-2026-01-22
- Reddit r/PMHNP. (2026, February 5). AI in Private Practice. https://www.reddit.com/r/PMHNP/comments/1qwvhor/ai_in_private_practice/
- The Permanente Medical Group / NEJM Catalyst. (2025). AI Scribes Save Physicians Time, Improve Patient Interactions and Work Satisfaction. https://permanente.org/analysis-ai-scribes-save-physicians-time-improve-patient-interactions-and-work-satisfaction/
- American Medical Association. (2024). Doctors Work Fewer Hours, But the EHR Still Follows Them Home. https://www.ama-assn.org/practice-management/physician-health/doctors-work-fewer-hours-ehr-still-follows-them-home
- Alpert JM, Saper R, Boose E, Ruff J, Hopkins K, Gaskins D, Guo N, Schneider JP, Giffi Scibona A, Gutierrez J, Rothberg MB. Evaluating an artificial intelligence scribe for clinical documentation. Digit Health. 2025 Nov 20;11:20552076251395588. https://pmc.ncbi.nlm.nih.gov/articles/PMC12638734/